
Faith discrimination in the NHS: multiple penalties facing Muslim doctors
Hina J Shahid, GP; Chairperson, Muslim Doctors Association
Published in JHH16.2 – Faith, hope and love for healthcare
Having a mixed heritage and growing up in three different countries made me curious and respect and accept differences from a young age. I was fed up with opening the newspaper every morning with headlines about male Muslim terrorists and oppressed Muslim women. I started doing community engagement work and working with the media to encourage dialogue, challenge prejudice and present an alternative narrative. Working in public health, humanitarian medicine and as a GP in an inner city practice have deepened my understanding of global, structural and social influences on health and healthcare institutions.The Dr Hadiza Bawa-Garba case really brought this home, raising uncomfortable questions about an institution I deeply cherish and that is regarded as a national treasure.
Introduction
The NHS is the fifth largest employer in the world and prides itself on its diverse values. BME staff make up 19% of the NHS workforce (Home Office, 2018). The NHS Employers diversity and inclusion team supports improved equality, diversity and inclusion within NHS organisations and one of the priorities listed for 2018/19 is to better understand wider faith and belief issues (NHS Employers, 2018). It is estimated that just under 10% of the doctors in the NHS are Muslim (NHS Digital, 2016). Belonging to a faith group has been demonstrated to support positive wellbeing, which is an asset in the current NHS climate with increasing levels of stress and burn out. However, there are concerns reported by Muslim doctors which have been amplified since the Dr Hadiza Bawa-Garba case; a landmark case that raised questions on religious discrimination in the NHS and associated regulatory and professional bodies.
British Muslims and Islamophobia – historical, social and political context
There are 2.8 million Muslims in the United Kingdom comprising just under 5% of the population. (Office for National Statistics, 2011). The presence of Muslims in Britain spans several centuries, and the influence of the Islamic world even longer in European arts, architecture, science, mathematics and philosophy. Research indicates that British Muslims feel a strong sense of religious identity, but that they are also more likely than the British public as a whole to say that their national identity as British is important to them. (Kaur-Ballagan et al, 2018)). A recent report shows that Muslims have the highest level of life satisfaction and wellbeing compared with other faith and non-faith groups (Edinger-Schons, 2019). Yet, there is depressing evidence demonstrating discriminatory outcomes faced by British Muslims in housing, education, employment, the criminal justice system, social and public life and political and media discourse, and that this has enormous social, economic and health consequences for society (All Party Parliamentary Group on British Muslims, 2018). More disturbing still is the increase in violence and hate crimes targeting Muslims in the UK. Muslim adults are more likely to be victims of racially motivated hate crime than other adults including those of other and no faith (Home Office, 2018). This continues to increase year on year with a consistent trend towards targeting Muslim women (Tell MAMA, 2017).
Although anti-Muslim sentiments and persecution in the west have a long history – whether as a pretext for medieval crusades, or for legitimising European colonialism – spectacular recent events that have intensified these sentiments into more conspicuous hatred and division in the public consciousness include Salman Rushdie’s Satanic Verses affair, the protests around the Gulf War, the 9/11 Twin Towers and London’s 7/7 tube bombings, home[1]grown Isis ‘jihadis’, ethnic and religious media stereotypes of a ‘clash of civilisations’, identity crises, poverty, criminality and political discourse linking Muslims with extremism and terrorism (Elahi and Khan, 2017). Here too, there is a notably gendered element, with a national poll revealing that 70% of the population perceives Islam as encouraging the repression of women and that wearing a headscarf is widely seen as symbol of this oppression (YouGov, 2010). These views are mirrored by the rise of nationalism and populism and growing support for far right and alt-right political groups.
This trend is particularly relevant for doctors. During the Dr Hadiza Bawa-Garba trial, a vitriolic smear campaign was launched against her by right-wing political groups and mainstream media and social media. Yet she was not offered any protection or support by her Trust, Royal College, General Medical Council or Higher Education England. A view widely held by front-line doctors was that Dr Hadiza Bawa-Garba, a visibly Muslim female doctor, was an easy target and scapegoat for the widespread systemic failures that contributed to her predicament.
Disgraced children’s doctor whose mistake led to the death of a six-year old boy is allowed to continue practicising medicine because she poses a low risk patients’
Whatever the term chosen – anti-Muslim hatred, anti[1]Muslim prejudice, Islamophobia – there is a pressing need for formal recognition of anti-Muslim hatred in all its manifestations. If Muslim healthcare staff are to be protected from violence and prejudice they need to be assured that transparent, accountable systems are in place in all private, public and civic spaces, and this must include especially the NHS and its associated regulatory, professional and employment bodies. The term Islamophobia was first coined by the Runneymede Trust in 1997 (Runneymede Trust, 1997) but it was only in 2018 that the All Party Parliamentary Group on British Muslims adopted a formal definition, which has since been accepted by the Labour Party and a number of cities in the UK. ‘Islamophobia is rooted in racism and is a type of racism that targets expressions of Muslim-ness or perceived Muslim-ness’ (All Party Parliamentary Group on British Muslims, 2018). The revised Runnymede definition of Islamophobia also has its roots in racism and similarly argues that the focus should be on people and perception rather than on ideas/ideology (Elahi and Khan, 2017).
Would you want a doctor convicted of manslaughter to care for YOUR child? How the colleagues of Dr Bawa-Garba who made fatal blunders in case of boy, six, want her to return to work
Religious discrimination and legislation in the UK
Development of anti-discrimination legislation in the UK has been reactive rather than proactive, prompted by broader national issues. The Equal Pay Act 1970, the Sex Discrimination Act 1975, the Race Relations Act 1976, the Disability Discrimination Act 1995, and the Disability Rights Commission Act 1999 (McClean, undated) have been mostly replaced by the more recent Equality Act 2010. The overlapping of race and religion makes them particularly difficult to disentangle, and all the more challenging to discern the specific and distinct impacts of religious discrimination. Although the Race Relations Act was passed in 1976 no effort was made to address religious discrimination until much later. Only in 2003, did the Employment Equality (Religion or Belief) Regulations make it unlawful to discriminate against those in vocational training and employment on grounds of sexual orientation and religion or belief. More general provisions were enacted in the Equality Act 2006, now replaced by the Equality Act 2010, whose guidance related to religion is shown below.
Equality Act 2010: Religion or belief
- Religion means any religion and a reference to religion includes a reference to a lack of religion.
- Belief means any religious or philosophical belief and a reference to belief includes a reference to a lack of belief.
- In relation to the protected characteristic of religion or belief:
- reference to a person who has a particular protected characteristic is a reference to a person of a particular religion or belief
- a reference to persons who share a protected characteristic is a reference to persons who are of the same religion or belief.
The Equality Act 2010 is very comprehensive and also provides guidance and recommendations for employers, which includes all public authorities under the public sector equality duty. The Act describes four types of discrimination: direct discrimination, indirect discrimination, harassment and victimisation as demonstrated in the box below. Additionally, the Act highlights key areas where discrimination by employers can occur: recruitment, taking time away from work for religious reasons, and dress code and appearance.
Equality Act 2010: Discrimination
- Direction discrimination – including ordinary direct discrimination because of a protected characteristic they protect, direct discrimination by association and direct discrimination by perception.
- Indirect discrimination – less obvious that direct discrimination and can often be unintended. It is where a criteria or practices is applied equally to a group of employees’ job applications but results in putting those with a shared certain protected characteristic at a particular disadvantage and the employer is unable to justify it.
- Harassment – can be verbal, written or physical and may include nicknames, threats, insults, jokes, ‘banter’, inappropriate questions, exclusion, inappropriate physical contact. 4
- Victimisation – where an employee suffers ‘detriment’ causing disadvantage, damage, harm or loss through raising grievances concerning equality or discrimination. Source: Advisory, Conciliation and Arbitration Service, 2018.
Institutionalising religious discrimination
Institutions and work environments are shaped by the geopolitical and social forces in which they operate. Research indicates that Muslims are the least likely social group to work in senior professional roles in the UK (Ali, 2015). Widespread Islamophobia, racism and discrimination, negative stereotypes, lack of Muslim role models, bullying and harassment are implicated as factors holding back Muslims in the workplace. (Stevenson et al, 2017). In particular, women wearing headscarves face worse discrimination in the workplace through experiencing the ‘triple penalty’ impacting on their job prospects: being female, being from an ethnic minority and being Muslim (Stevenson et al, 2017 and House of Commons Women and Equalities Committee, 2016). Unfortunately, these trends also filter down to healthcare institutions.
Research on racial disparities for healthcare staff has consistently demonstrated clear differences in attainment, for instance the relative lack of BME representation in leadership positions, along with a worrying trend of increasing discrimination against BME staff and that a high proportion are affected by formal disciplinary process (NHS Equality and Diversity Council, 2018). BME doctors are more likely to be complained about, be investigated and to have higher sanctions imposed on them. They are also more likely to be disciplined, to fail their postgraduate exams and to be erased, suspended and/or face criminal conviction (Humphrey et al, 2011; NHS England, 2017; Esmail and Roberts, 2013). Research on actual religious disparities in the NHS is an area of increasing interest, though as yet evidence is scarce. A King’s Fund Report demonstrated that healthcare staff from all religions experience discrimination on the basis of their faith, but by far the highest is towards Muslims (West et al, 2015). It is therefore not surprising, but still depressing, that despite making up approximately 10% of the medical workforce, only 2.5% of managers and 1.7% of senior managers are Muslim (NHS Digital, 2016).
Additionally, various work policies, which have been highlighted as potentially institutionally anti-Muslim, may contravene equality legislation. The Prevent policy has been accused of contributing to stereotypes that link Muslims with terrorism. It has been cited as causing moral distress among doctors, especially Muslim doctors, who view it as a racist policy which, exacerbated by structural issues in the NHS, and by politicising and securitising the NHS work environment, create an atmosphere of fear, distrust, self-censorship, reluctance to vocalise dissent or concerns around freedom of conscience (Younis and Jadhav, 2019).
Trusts’ dress code policies are an area of concern where science, safety and religion potentially conflict. For instance the ‘bare below the elbows’ policy, that links work clothes with transmission of infection, is bound to create difficulties for female Muslim doctors, and in some cases, may prevent them from pursuing a career in hospital medicine and surgery (Malik et al, 2019). Additionally, as trusts have no consistent policies about headscarves in operating theatres, women wearing the headscarf face discrimination in surgical jobs such as breast surgery and obstetrics and gynaecology, specialties desperate for female doctors.
Individual experiences and intersectionality
International studies have shown that American Muslim doctors on the front line report feeling greater scrutiny at work, religious discrimination and lack of career progression (Padela et al, 2016). In Canada, Muslim female health professionals report a lack of support from management, being judged by colleagues, social pressures affecting wellbeing, perceived incompetence and a lack of acceptance by colleagues and patients (Siddiqui, 2012).
A recent report highlights the growing pressures facing ‘disillusioned’ NHS staff causing low morale, feelings of stress and burnout and leading to exodus of staff and a deepening workforce crisis (NHS England/Improvement, 2019). If in addition institutional and environmental elements are working against them, this may add to stress and fuel burnout. A rapid review conducted by the Muslim Doctors Association (Shahid and Abdulkareem, 2018) confirmed the ‘triple penalty’ observed in other sectors. However, further narrative reports currently being collected as part of more formal research indicate that discriminatory systems are more complex. Through the lens of intersectionality one can see how ‘layer after layer of inequality’ intersect to increase vulnerability and discrimination faced by Muslim doctors who have multiple protected characteristics as defined by the Equality Act 2010 (Wiley, 2018). Some quotes – all from female Muslim doctors – have been extracted from narrative accounts currently in collection,
The registrar would bleep me several times on purpose after I told him I was going to go to pray and be back in 10 minutes. When I’d return I’d see him laughing and saying “that was a long prayer, didn’t God tell you that you have jobs to do?
Foundation year one doctor
Although I have rarely experienced overt prejudice mine is more subtle. It’s the assumption through the questions from others that I don’t speak English, it’s the lack of friendliness during induction in new jobs where I don’t know anyone, it’s the assumption that I don’t know the system or am new to the UK or am not in a training programme, it’s the assumption that I will not be able to do my job well and the constant having to prove myself with each new rotation. It’s the eye rolling from the nurses and seniors when asking questions, it’s the surprised reaction that actually I am a normal human being’ who is relatively competent at her job with outside interests and hobbies
Paediatric specialty trainee year 6 doctor
You can’t wear that thing in theatre” (said the consultant while pointing at my scarf in front of the scrub nurses and registrar). I removed by headscarf and put a surgical cap over my head. “There. Much better. No need to wear a rag on your head all of the time is there?
Foundation year two doctor
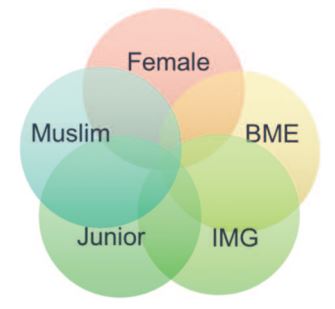
Gender inequality is a reality for women in medicine, for they experience under-representation in leadership positions, academia and competitive medical specialties, and a gender pay gap (Rimmer, 2017). Most Muslim doctors in the NHS are from BME backgrounds and so face these obstacles as well as the racial disparities already discussed. The narrative accounts confirm these gender and racial disparities but indicate too that being ‘visibly’ Muslim (wearing a headscarf), being an international medical graduate, and being a junior doctor further increase vulnerability and risk of discrimination (Figure 1). The narrative accounts highlight the day-to-day challenges and assumptions faced by female Muslim doctors and the feeling of not belonging in the team. Other consistent themes emerging from narrative reports include negative stereotypes and prejudice, intimidation, harassment and bullying, lack of acceptance by colleagues, issues with career progression and academia, lack of formal support around raising concerns, and negative impact on stress and wellbeing. However, despite the impact that religion may have on experiences of Muslim doctors working in the NHS, faith remains a strong part of the identity of Muslim doctors and an important means of coping with stressors and adversities. It is therefore imperative not just to tackle the problems Muslim doctors face but also to support faith practices proactively and the beliefs that form such a core part of their identify and sense of wellbeing.
Looking ahead
Awareness of these challenges and the work that needs to be done presents the NHS with important opportunities. The NHS Employers diversity and inclusion team has expressed its commitment to better understand wider faith and belief issues (NHS Employers, 2018). This is also reflected in the NHS Long Term Plan’s pledge to ensuring diversity in leadership, recognising as it has, that a diverse workforce at all levels will lead to increased organisational efficiency and improved patient outcomes (NHS, 2019). Improved collection on faith data is necessary as a first step, with a view to creating a faith equality index, similar to the race equality index, which would improve monitoring of diversity, inclusion and representation of Muslim doctors across NHS organisations. It is misleading for organisations to state that they are truly diverse and inclusive when doctors feel unable to practise their faith freely and ‘bring their whole selves to work’. Further studies need to be conducted to explore the prevalence and impact of unconscious bias, the religious discrimination faced by NHS staff working on the frontline, and the attitudes of management and policy leaders
There is a need for improved awareness, dialogue and processes for tackling religious discrimination and improving faith equality. This could be done through collaborative engagement between the relevant organisations in the field of faith, regulation, professional accreditation, academic and training bodies, and employment institutions. Importantly, work environments need to adopt a zero tolerance policy towards racial and religious discrimination and to ensure improved training and awareness of cultural and faith-sensitive issues. There is a need to design and implement safeguards that allow staff to report concerns around religious discrimination in a safe environment. Support structures for affected colleagues and effective policies can ensure escalation of complaints and timely and proportionate action. A greater presence of Muslim mentors and role models in leadership positions and in competitive specialities and academia would provide aspiration and inspire hope in young doctors and demonstrate NHS commitment to equality, diversity and inclusion.
Conclusions
There are moral, legal, economic, health and patient safety arguments for better inclusion, representation and support for doctors from Muslim backgrounds, who despite making up a sizeable minority of the NHS work[1]force, are under-represented at senior levels and report experiences of discrimination, prejudice and harassment. These are consistent with trends seen internationally and in other institutions in the UK, and appear to reflect widely held negative social attitudes. Concerns reported by Muslim doctors include structural barriers – lack of representation at leadership levels, institutional policies such as Prevent and dress codes and individual experiences of career progression, negative stereotypes, exclusion and difficult team dynamics, and barriers to practising faith at work. Additionally, these concerns indicate that in the NHS multiple penalties exist against doctors who are female, BME, Muslim, international medical graduates and in junior grades. Combined, these factors produce worse layers of inequality when compared to other employment sectors. Further research and evidence-based vertical and horizontal policy approaches are needed to understand and achieve improved faith equality for Muslim doctors working in the NHS.
References
- Advisory, Conciliation and Arbitration Service (2018) Religion or belief discrimination: key points for the workplace. London: ACAS.
- Ali S (2015) British Muslims in numbers. London: Muslim Council of Britain.
- All Party Parliamentary Group on British Muslims (2018) Islamophobia defined: the inquiry into a working definition of Islamophobia. London: All Party Parliamentary Group on British Muslims.
- Edinger-Schons LM (2019) Oneness beliefs and their effect on life satisfaction. Psychology of Religion and Spirituality [online] 11 April.
- Elahi F, Khan O (eds) (2017) Islamophobia: still a challenge for us all. London: Runneymede Trust.
- Esmail A, Roberts C (2013) Academic performance of ethnic minority candidates and discrimination in the MRCGP examinations between 2010 and 2012: analysis of data. BMJ 347, f5662.
- Home Office (2018) Hate crime, England and Wales 2017/18. London: Home Office.
- Humphrey C, Hickman S, Gulliford MC (2011) Place of medical qualification and outcomes of UK General Medical Council ‘fitness to practise’ process: cohort study. BMJ 342, d1817.
- Kaur-Ballagan K, Mortimore R, Gottfried G (2018). A review of survey research on Muslims in Britain. London: Ipsos Mori Social Research Institute.
- Malik A, Qureshi H, Abdul-Razakq H et al (2019). I decided not to go into surgery due to dress code: a cross-sectional study within the UK investigating experiences of female Muslim medical health professionals on bare below the elbows (BBE) policy and wearing headscarves (hijabs) in theatre. BMJ open 9(3) e019954.
- McClean D (undated) [online] Religion and discrimination in the United Kingdom. Available at: www.law.cf.ac.uk/clr/research/Oxford – United Kingdom.pdf (accessed 23 April 2019).
- NHS Digital (2016) Hospital and Community Health Services (HCHS) workforce statistics: equality and diversity in NHS Trusts and CCGs in England. London: NHS Digital.
- NHS England (2017) Improving through inclusion: Supporting staff networks for black and minority ethnic staff in the NHS. London: NHS England.
- NHS England (2019) The NHS Long Term Plan. Leeds: NHS England.
- NHS England/Improvement (2019) Interim people plan. Available at: https://improvement.nhs.uk/resources/interim-nhs-people-plan (accessed 23 April 2019)
- NHS Employers (2018) Diversity and inclusion [online] Available at: www.nhsemployers.org/your-workforce/plan/diversity-and-inclusion (accessed 23 April 2019).
- NHS Equality and Diversity Council (2018) NHS workforce race equality standard: 2018 data analysis reports for NHS Trusts. London: NHS Equality and Diversity Council.
- Office for National Statistics (2011) Religion in England and Wales 2011. Available at: www.ons.gov.uk/peoplepopulationandcommunity/ culturalidentity/religion/articles/religioninenglandandwales2011/2012- 12–11 (accessed 23 April 2019).
- Padela AI, Adam H, Ahmad M, Hosseinian Z, Curlin F (2016) Religious identity and workplace discrimination: A national survey of American Muslim physicians. AJOB Empirical Bioethics 7(3) 149–159.
- Shahid H, Abdulkareem B (2018) The triple penalty: Muslim doctors in the NHS. Muslim Doctors Association
- Siddiqui A (2012) Experiences of Muslim women as healthcare professionals in Canada. [online thesis]. Available at: https://pdfs. semanticscholar.org/4152/badfcd6dcd7b1d32e92a6bdc06d1f90f3dce. pdf (accessed 23 April 2019)
- Stevenson J, Demack S, Stiell B et al (2017) The social mobility challenges faced by young Muslims. London: Social Mobility Commission.
- Stevenson J, Demack S, Stiell B et al (2017) The social mobility challenges faced by young Muslims. London: Social Mobility Commission.
- West M, Dawson J, Kaur M (2015). Making the difference: Diversity and inclusion in the NHS. London: The King’s Fund
- Wiley E (2018). Layer after layer of inequality. London: British Medical Association.
- YouGov (2010). Exploring Islam: foundation survey results. London: YouGov
- Younis T, Jadhav S (2019) Keeping our mouths shut: the fear and racialized self-censorship of British healthcare professionals in PREVENT training. Culture, medicine, and psychiatry 1–21.



{kind=link}
{kind=link}
{kind=link}
{kind=link}