

Realistic hope – and its role in keeping us resilient in times of crisis
Catherine Zollman, GP; medical director, Penny Brohn UK
Jennie Evans, Advanced cancer patient and Penny Brohn UK client
Published in JHH16.2 – Faith, hope and love in healthcare
I first became interested in holistic approaches to health as a medical student lucky enough to join the BHMA in its early days. I trained initially in medical oncology and immediately saw the potential of an approach that combined lifestyle support, conventional treatment and complementary therapies, even though the term integrative oncology hadn’t yet been invented. I now work at Penny Brohn UK, the leading charitable provider of complementary and lifestyle support for people with cancer, as well as continuing my part-time NHS GP and university teaching work.
Catherine Zollman
I was diagnosed with Stage IV colorectal cancer on the 2 September 2015. On 21 September 2015 I walked through the doors of Penny Brohn UK for the first time, seeking to find out how I could help myself in the face of the cataclysmic life change I was experiencing. In the face of a now incurable diagnosis, I have learned to navigate as meaningful a path through the minefield of life with cancer as I can with the continued support of PB, and I now try to share my experience in the hope that it might help others.
Jennie Evans
‘What is the most helpful way to think about the future?’
This question may seem rather abstract and philosophical, but if you are dealing with a potentially life[1]limiting condition, it has a very practical and profound influence on everyday life.
In our work at Penny Brohn UK, a charity which provides free holistic support and education to people affected by cancer, we grapple with this question daily, whether we are staff or clients. Many people are now supporting someone or living with a cancer diagnosis themselves. We’re living at a time where more people are being diagnosed, and often at a younger age, than ever before, but more are also living longer with the disease. It’s an area where positive psychology messages abound, and the ‘breakthrough treatments’ that seem just around the corner are still not a reality for most people. The connections between what we think or feel and our physical health are scientifically ever more convincing, so it feels as if there has never been a time when the answer to this question has been more relevant. We have started talking about ‘realistic hope’ as a way of helping people to navigate the present in a way that is grounded in reality, while enabling them to feel positive about life and the future, whatever that may hold.
[bctt tweet=”Humans have an innate need for connection, whether this is to or through other people, animals, nature, music, art…” username=”BritishHolistic”] In this article, we explore aspects of realistic hope, and the factors that influence it, from two contrasting stakeholder perspectives: an integrative medical doctor working with people affected by cancer at Penny Brohn UK (CZ), and someone living with advanced cancer, who has used the services at Penny Brohn UK to help develop and foster realistic hopefulness (JE). We have based the thoughts that follow on a conversational exploration of Jennie’s lived experience and Catherine’s years of clinical work in this field. We have chosen this observational and experiential style, rather than a literature-based review, with the aim of highlighting some of the more complex and subtle attributes and nuances that may enable individuals to move forward and hold their balance on the delicate tightrope of realistic hopefulness.
Hope is the thing with feathers That perches in the soul And sings the tune without the words And never stops at all
And sweetest in the gale is heard And sore must be the storm That could abash the little bird That kept so many warm.
I’ve heard it in the chillest land, And on the strangest sea; Yet, never, in extremity, It asked a crumb of me. Emily Dickinson 1830–1886
What is ‘realistic hope?
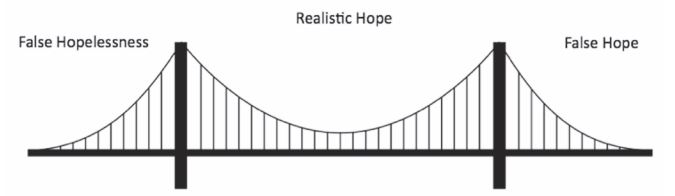
Realistic hope, if one can maintain it, is a delicate tightrope to walk, the ‘sweet spot’ between the two polarised and limiting extremes of false hope and false hopelessness. When faced with a potentially life-limiting condition, it’s common for people to feel a huge sense of grief for the future they had always assumed was theirs for the taking, for the ‘life that was’. Like other forms of grief, this can sometimes manifest as denial. This kind of false hope refuses or is unable to accept that the future is going to be different from how one wants or imagined it to be, a belief that somehow there is a way back to that previously expected future. For others, where the loss of their expected future may end up being confused with the loss of any future (false hopelessness) it can manifest as depression. Both of these expressions can disable a person’s ability to move beyond grief, and will often prevent them from finding joy, meaning and connection in the rest of their lives.
For many who cannot see hope, their vision is blurred because they believe they are unable to exert any control over their circumstances.’ ‘
False hope is an insubstantial foundation on which to stand and weather the vicissitudes of difficult circumstances
Jerome Groopman, Anatomy of Hope (2003)
Definitions of realistic hope
If someone living with cancer can develop ‘hope without an attachment to a specific outcome’ it will allow them, though they may fail to realise a specific goal, still to hold on to the core of hopefulness that is so integral to well[1]being, and which Emily Dickinson so perfectly describes in her poem, above. For us goal-orientated, future-fixated humans to achieve this non-attachment to a fixed outcome, while remaining deeply invested in reaching the best outcome possible in the circumstances, is undeniably difficult, but it is perhaps the pinnacle of realistic hopefulness.
Healthcare professionals helping patients or clients to find realistic hope, will have to support them compassionately as they come to understand and accept the uncertainty of their future and the many potential scenarios that might unfold. At the same time they will need to help them find reasons to be hopeful about life itself as precious and worthwhile. The various and ambiguous futures will not only include best and worst case scenarios but also some more probable outcomes. Each of these scenarios needs to be held as a genuine possibility, and discussed by the individual and their healthcare team as there may be important ways that they can exert some influence over which version of the future eventually unfolds.
What does realistic hope look like?
Different people express their experiences of realistic hope in different ways. Some appreciate the difference between ‘probability’ and ‘possibility’, and find they can focus on ‘possibility’ in ways that open up a broader, more creative and dynamic relationship with the future. Some rediscover a more peaceful, balanced perspective where they feel more connected and more loving and compassionate towards themselves and the world. They may talk about coming to understand the difference between ‘healing’ and ‘curing’. For others realistic hope with its myriad branching possibilities and opportunities for change and post-traumatic growth brings a greater sense of aliveness and energy to everyday life.
Hope is like the sun, which, as we journey toward it, casts the shadow of our burden behind us
Samuel Smiles, 1812–1904
A key factor in finding realistic hope seems to be an acceptance of reality with its inherent lack of true certainty about anything other than the present moment. The ability to appreciate and find meaning and value in living each day also seems to help people to stay realistically hopeful, even in the face of tragedy, extreme challenge or approaching death. We have summarised and explained these and the other six factors we have found most relevant below.
Eight key aspects of realistic hope
- Acceptance
- Appreciation
- Holistic outlook
- Sense of control
- Resilient thinking
- Connection • Motivation
- Background resilience
Acceptance
Realistic hope does not require people to ‘be positive’, rather it arises when people accept their current situation, including their thoughts and emotions, without judgement but also without feeling defined by them or overly[1]attached to them.
Appreciation
Realistic hopefulness often involves a greater appreciation of the value of everyday experiences, both positive and negative – finding a reflective appreciation of both the ‘life
I had before’ and the ‘life I have now’ without falling into the trap of comparing one unfavourably with the other. The richness this brings seems to come with a sense of life as a gift, and of each moment lived with good intention as a bonus. On the other if someone feels aggrieved or ‘robbed’ of their ‘right’ to a fixed outcome this can make it harder to find hope and resilience.
Holistic versus mechanistic outlook and a focus on possibility versus probability
Statistical information like average life expectancy for a particular cancer can help people understand more about their likely prognosis, come to terms with their situation, and make certain decisions about treatment. However, the use of statistics in healthcare is predicated on a Newtonian view where the assumption is that if a study sample is big enough, people with similar demographics and cancer characteristics come to be seen as identical ‘billiard balls’ for whom average survival times will generally apply. For this Newtonian, deterministic mindset, the human body is subject to a linear, easily predictable progression of events, and the things that determine our health or otherwise are largely outside our control. An example would be the genetic theory of carcinogenesis whose natural conclusions tend to encourage fatalism (‘I have incurable cancer, so my lifespan will be whatever the stats predict’). David Servan-Schreiber (2011), a doctor and a cancer patient, describes how he escaped the ‘tyranny of statistics’. Whereas some people find themselves ‘counting down their days’ according to the survival rates they have been given, people, like him, who find realistic hope often adopt a more holistic mindset. They instead consider that what happens to their body is far less predictable and depends on emergent properties, which are more than the sum of their individual parts. According to the science of epigenetics, not all of the genetic messages written in our DNA are actively expressed, and the choice of messages which end up being selectively expressed is very much affected by lifestyle, social and environmental factors. Another relevant developing science is affective immunology (D’Acquisto, 2017), which studies the inter-relationships between our immune system and our emotional health. The complex interactions between our microbiome and our immune system is yet another example of a research area where there is a growing appreciation of more complex, evolving mind–body– environment dynamics. These post-Newtonian perspectives can give us a broader view of potential individual possibilities as opposed to averaged group probabilities.
When you change the way you look at things, the things you’re looking at change.
Max Planck, physicist, 1858–1947
Control
From Jennie’s perspective, having some element of control is important in maintaining her realistic hopefulness. She describes how when she feels powerless, Realistic hope – and its role in keeping us resilient in times of crisis REALISTIC HOPE 26 © Journal of holistic healthcare ● Volume 16 Issue 2 Summer 2019 this contributes to her feeling more hopeless and that the reverse is also true. Feeling hopeless contributes to a sense of helplessness, and it is hard to maintain one’s hope without feeling somewhat in control. Appraising all the relevant options leads to better, more informed joint decision-making and therefore a greater sense of control. However, being realistically hopeful does not necessarily mean becoming involved in every shared treatment decision: in fact making an active choice to trust and not to question medics may be equally valid. With a holistic outlook the notion of healing (becoming more whole), as opposed to curing (getting rid of a symptom or disease), becomes something to hope for and something which is often more under an individual’s control.
The future depends on what you do in the present
Chöje Akong Tulku Rinpoche, Kagyu school of Tibetan Buddhism tulku, 1930–2013
Resilient thinking
A growth mindset (Dweck, 2017) is a way of thinking about the future, which is conducive to finding realistic hope. A fixed mindset on the other hand encourages fatalism in the face of what becomes a seemingly hopeless situation. People with growth mindsets take in the full range of possible outcomes, including the best and worst situations that may arise, and then focus on what can be done to make a better outcome a little more likely. Dr Chris Johnstone (2019) describes this as flexible or resilient thinking. Resilient thinking also involves noticing that all along our lives there are ‘choice points’, where a number of factors, some of them under our control, influence ‘what happens next’, so that we are not necessarily trapped by our past or by our present.
You can often choose your path, even in the final stages of illness
Pat Pilkington (2016)
Connection
When we feel realistically hopeful, all potential eventualities can be discussed and it becomes more possible to connect and have ‘important conversations’ with the people that matter most. Connection is a key part of healing and thriving as a whole person. Kathryn Mannix and Atul Gawande both describe how our current ‘Age of Denial’ inhibits such important conversations, as people fear that the emotions and thoughts they are experiencing, but keeping a lid on, will be too upsetting for themselves and others to handle. The good news is, that once people do start having and benefitting from these conversations, it often gives others permission to do the same.
Humans have an innate need for connection, whether this is to or through other people, animals, nature, music, art, a deeper purpose, or something bigger than themselves. Jennie describes below how realistic hope can connect her with the present moment. Even if this involves a greater awareness of pain or difficulty, it can still enable her to be more authentic and more able to connect with others. Though denial can be a useful tool for some people, as Kathryn Mannix (2017) describes in one of her case studies, it is potentially damaging when driven by a fear of facing reality. This isolation and separation from others who may see a different version of the future can eat away at support, and can erode any truly shared enjoyment or experience of the ‘now’. Realistic hope enables people to prepare together for the worst and hope for the best, and can make it easier to explore different options with curiosity and purpose, redefining and adapting what it is that one is hoping for as life evolves.
Motivation
There is a fine line between hope and motivation. There is no question that having something to hope for, to aim at, is helpful when faced with cancer, and particularly when faced with a terminal diagnosis. There are thousands of stories of people who survived longer, so they could live to see their child born, daughter married, son graduate etc, but then died immediately afterwards. Though milestones held lightly can be useful to aim for, there are also many stories of people who weren’t able to reach them. So maintaining motivation without a specific target date offers more freedom to enjoy what there is in the here and now, without a sense of pressure, failure, guilt or self-blame.
Background holistic resilience
At Penny Brohn UK we use the Bristol Whole Life model (www.pennybrohn.org.uk/wp-content/uploads/2017/01/ General-Brochure-final-online.pdf) to help people reflect on their physical, psychological, emotional, social and spiritual resilience. People with a strong base of resilience in several of these areas seem to find realistic hopefulness easier to access. The shock of a cancer diagnosis can be profoundly destabilising and disabling. Whole life resilience helps people feel ‘safer’ by reducing the anxiety of flight and fight, or by pulling them out of despair and collapse. At Penny Brohn UK, in order to help people regain a deeper sense of security and wellbeing, we encourage good nutrition, physical activity, better sleep and relaxation, good symptom management, and provide the emotional and psychological support that can calm the body’s threat responses and nurture trusting, loving and meaningful connections.
Attaining realistic hopefulness – Jennie’s perspective
Arriving at a place of realistic hopefulness takes time. Just how long depends on an individual’s circumstances, culture, age, and personality.Activities at Penny Brohn UK aim to calm and relax people so they can begin to see the possibility of realistic hopefulness. In developing appreciation for ‘what is’ and coming to feel realistic hopefulness, mindfulness is a fundamental tool. But it is important for some people – particularly those like me – to understand that acceptance and surrender, and attaining Zen-like calm and quietness, are not the only routes. Hoping is actually an energetic practice, and I find activities that generate energy are equally valuable, whether gentler pursuits like art or more active ones like walking or dancing.The important aspect is that the energy expended in the activity is less than the energy generated by it, whether mental, emotional, physical or spiritual energy.When it is, and the flow of energy is restorative and completing, it enables Emily Dickinson’s ‘bird in the soul’ to sing ever more loudly.
What stops people achieving realistic hopefulness?
As described above, realistic hope can be a useful perspective for people living in challenging situations, but for many it remains an elusive state. Why is this? A number of cultural, societal and practical barriers can get in the way in today’s world. Many of them are being addressed slowly by pioneering individuals who are looking for better ways to help themselves or other people stay resilient.
Eight key barriers to achieving realistic hopefulness
- Culture
- Exaggerated claims about treatment
- Medical pessimism
- Attitudes of friends and family
- The complementary/conventional divide
- Tyranny of the positive • Unaddressed fears about death
- High levels of unmanaged distress
Culture
Autonomy has gradually become a key concept in the doctor–patient relationship. However, truth‐telling is far from being the norm in many countries in the world, despite widespread general agreement on the benefits of open communication between physicians and cancer patients. In many cultures there is still strong resistance against disclosure of diagnosis and prognosis in cancer and other life-limiting conditions (Shahidi, 2010). Yet without truthful communication, realistic hopefulness is almost impossible to achieve and may not be a feasible, or even a desirable goal. Cultural sensitivity is essential, but culture should not be used as an excuse to make general assumptions about the appropriateness of concealment of prognosis. Individual preferences need be elicited, particularly where people are exposed to more than one culture.
Exaggerated claims about treatment
Often fuelled by the media, and exponentially increasing online information and social media, exaggerated claims abound. News (and fake news) of new or unconventional treatments can lead individuals to focus exclusively on the search for a cure, at the expense of accepting and addressing the reality of their situation. Alternative practitioners, as well as pharmaceutical companies and mainstream healthcare professionals, sometimes overstate the likely benefits and downplay risks. A degree of scepticism is justified whether towards ‘an ancient traditional discipline for strengthening the body and correcting underlying imbalances to eliminate cancer naturally’ or ‘a break[1]through new pharmaceutical agent that will be a potential major advance in targeting cancer cells’.
Medical pessimism
Patients with advanced cancer find it easier to remain hopeful if their oncologists are confident, collaborative, realistic and supportive and are prepared to give detailed information about prognosis and discuss a variety of options (Hagerty et al, 2005). However, many Penny Brohn UK clients (from all around the UK) still describe disempowering and patronising encounters where they felt hope was crushed by oncology professionals who repeatedly emphasised the incurable and progressively terminal nature of cancer. Perhaps the motive stems from a fear of raising unrealistic expectations and fuelling false hope, particularly when someone asks about complemen[1]tary or lifestyle approaches that an oncologist might worry will lead ‘their patient’ to reject conventional treatment. This sort of disempowering message and the breakdown in the doctor-patient relationship that often follows can have an anti-placebo (or ‘nocebic’) effect. If as a result a patient becomes depressed (depression is associated with increased mortality) or hopeless or, having been told that lifestyle was irrelevant, adopts unhealthy behaviours, this could result in a self-fulfilling worsening of prognosis. That being said, many oncologists and GPs are acutely aware of and skilled in their role of facilitating a helpful, realistically hopeful attitude in their patients – see below
Consultant medical oncologist perspective
When patients hear they have cancer, they’re faced with a bewildering amount of information – some helpful, some less so. Beyond everything, in this confusing array of advice and anecdotes, patients look for hope.As an oncologist, it’s important for me to help patients and their loved ones navigate this new complex world they find themselves in – and to find realistic hope and goals. In my experience, this helps bring positivity which in turn helps patients cope with the many, many trials and tribulations of having cancer treatment and ultimately get the best out of their treatment.
GP perspective
To me, hope is not only based on everything being great, but ‘being hopeful’ means that whatever life throws at us we trust we will be supported and not alone. Encouraging hope is crucial to being a GP as you are letting patients know that you are with them and there for them and that what we hope for through an illness may change from cure to symptom management and that that is all OK
Attitudes of friends and family
Just as it is difficult to maintain realistic hope if healthcare professionals are either overly optimistic or overly pessimistic, it can be difficult if people who are close to you have a different way of dealing with the future. Sometime a person with a diagnosis of cancer is ready to have ‘important conversations’ but their friends and family are not. Sometimes it is the other way around. In either case, it is difficult to maintain realistic hope on your own, so connecting with others in similar situations through books, social media and the internet and hearing from other people living with life-limiting disease who ‘tell it how it is’ and still manage to find joy, meaning and fulfil[1]ment can be inspirational (Sabbage, 2017; You Me Big C Podcast, 2018–2019).
The complementary/conventional divide
Hostility between the worlds of conventional and complementary medicine can fuel false hope. Vulnerable and confused people without easily available and reliable sources of balanced unbiased information are often forced into a polarised, black and white, ‘either/or’ situation where they feel they must choose to pin their hopes on one approach to the exclusion of the other. Independent integrative practitioners who are trained in lifestyle approaches as well as both conventional and complementary disciplines can be very helpful in helping people bridge this divide and supporting them to get the best of both worlds.
Tyranny of the positive
While there is hard science that demonstrates the inter[1]connections between mental and physical wellbeing and confirms the potential of the placebo effect to significantly alter physical health parameters (Marchant, 2016) there are schools of thought that take this to the extreme and suggest that ‘if you 100% believe in an outcome, you can make it happen’. This has the obvious corollary that ‘you are responsible if you don’t get that outcome’ and that ‘acceptance of your situation = giving up’. From the perspective of someone like Jennie, who is living with advanced cancer ‘this attitude/belief exaggerates our own importance, power and control over our destiny and can put a huge weight of responsibility on our own shoulders that can be crushing and very tiring to carry.’
[false hope can be fuelled by] ‘glib assertions… that the power of the mind is limitless in influencing the clinical outcomes of virtually all diseases’.
Groopman, 2003
Unaddressed fears about death
In our ‘age of denial’ (Mannix, 2017) about death and dying many of us find the topic profoundly disturbing because we lack the skills and experience to discuss it wisely and openly. An honest appraisal and acceptance of all potential outcomes is an essential element of living with realistic hope, so as long as one (eventually inevitable) outcome is effectively a taboo subject, and cannot be fully explored, a sustainable state of realistic hope remains unattainable. Thankfully, many useful publications and initiatives are attempting to address this (see the useful resource section at the end of Mannix, 2017)
High levels of unmanaged distress
In acute distress when the sympathetic nervous system is in overdrive, the fight/flight mechanisms are triggered. This resulting changes in brain chemistry and physiology make clear judgement more difficult and ‘toxic thinking’ more likely. Examples of these ‘cognitive distortions’ include ‘black and white’ thinking, over-generalisation and catastrophising, that can drive a person towards giving up (false hopelessness), or a grasping at straws (false hope). The underlying distress could result from very practical concerns about finances, work or domestic commitments, or be due to physical disturbances – pain, severe symptoms from cancer or cancer treatments, sleep disturbance, malnutrition etc. The distress might also have more psycho-emotional, existential or spiritual dimensions. Holistic assessment and support, education about self[1]management and good symptom control will all be necessary before people can get to a place where they are able to start thinking realistically about the future with a more balanced perspective. People need to be helped to feel ‘safe enough’ before they have any chance of finding realistic hope.
Living with and without realistic hope – Jennie’s perspective
It is fairly obvious when someone else has unrealistic hopes, particularly when these are related to their state of health (eg hoping to run a marathon again when already confined to a wheelchair as a result of a progressive illness) but it may be harder to spot when we ourselves have unrealistic hopes or expectations. Broader, generic hopes may or may not be realistic, eg finding a cure for cancer, depending on the degree of specificity – finding a cure in time to cure me, or finding a cure eventually.
The opposite side of unrealistic hope is also potentially damaging. Many people describe depression as feeling hopeless. Focusing purely on what can be a very grim prognosis/reality can be very depressing indeed.As human beings, particularly in the first world, it is very difficult for us not to live in the future tense – our life runs around plans for next week, dental appointments six months off, booking your holiday for next year. Losing our ability to live in the future can be both disorientating and distressing, and is exacerbated where that future seems completely preoccupied with treatment, declining health and, ultimately death. Having no hope can lead, quite literally, to giving up on life.
As well as freeing me from needing a specific outcome so that I can be ‘OK’ with the possibility of dying, realistic hopefulness enables me to plan in a practical way, even though I still retain the hope that, with an integrative approach to my treatment, my death is not an imminent inevitability. In my view, this is an important part of being at peace with myself and my life. It includes putting in place an Advanced Care Plan, writing down wishes for my funeral arrangements and making sure I spend quality time with certain people.
From a place of realistic hopefulness, I feel able to experience the full range of emotions, to feel whole and exquisitely alive because there is no barrier of my own making between me and the world. Unrealistic hope and/or hopelessness, by definition, would close parts of me to myself, others and the beauty of the moment, and would allow me to get lost in worlds that exist only in my mind, places that others around me cannot go to, and that would separate us at a time when connection is most important.
The physical impact of realistic hope
Many studies have shown that hopefulness can have a direct beneficial impact on physical health and biological health markers (such as immune system response, cortisol profiles, and cardiovascular function) as well as the more obvious impact on mental health and likelihood of making positive lifestyle changes (Conversano, 2010; Dockray, 2010). Studies in people with cancer report that those who have an optimistic outlook have a better quality of life and improved mental wellbeing compared to pessimists. However, the results of studies looking at whether this is linked to improvements in survival are mixed (Schulz, 1996; Allison, 2003; Schofield, 2004) so, once lifestyle factors are taken into account there is as yet no clear large-scale evidence in cancer populations as a whole, to link any particular mental attitude or personality type with improved survival. However intriguing research into the small but well-documented number of people who experience a spontaneous or radical remission from cancer suggests that ‘taking control’, which depends on a level of hopefulness, may be one of the key factors responsible for their unexpected wellbeing. More careful research is needed to help unravel the complex and individual nature of realistic hope, and the physical effects it may have, including whether it can help some people with cancer live longer as well as better.
Summary
Developing and nurturing realistic hopefulness in our clients is core to the work of Penny Brohn UK and a key foundation for enabling them to live well with cancer. Understanding what Realistic Hopefulness looks like from a client perspective, the factors that encourage or prevent it, the difference it can make both psychologically and physically, and the role conventional and complementary medicine practitioners may play in this is, we believe, vital to the success of an integrative approach to cancer patient care.
I see hope as the very heart of healing. For those who have hope, it may help some to live longer, and it will help all to live better
Jerome Groopman, 2003
References
- Allison PJ (2003) Dispositional optimism predicts survival status 1 year after diagnosis in head and neck cancer patients. J Clin Oncol 21, 543–548.
- Conversano C (2010). Optimism and its impact on mental and physical well-being. Clinical practice and epidemiology in mental health 6, 25–29.
- D’Acquisto F (2017) Affective immunology: where emotions and the immune response converge. Dialogues Clin Neurosci. 19 (1) 9–19.
- Dockray S (2010) Positive affect and psychobiological processes. Neurosci Biobehav Rev. 35 (1): 9–75.
- Dweck C (2017) Mindset (6th ed). London: Robinson.
- Gawande A (2015) Being Mortal. London: Profile Books.
- Groopman J (2003) The anatomy of hope. New York, NY: Random House Books.
- Hagerty R et al (2005) Communicating with realism and hope: incurable cancer patients’ views on the disclosure of prognosis. Journal of Clinical Oncology 23 (6) 1278–1288.
- Johnstone C (2019) Resilience. London: Little Brown.
- Mannix K (2017) With the end in mind. Glasgow: William Collins.
- Marchant J (2016) Cure: a journey into the science of mind over body. Edinburgh: Canongate Books.
- Pilkington P (2016) The golden thread: a quiet revolution in cancer care. London: Jessica Kingsley.
- Sabbage S (2017) The cancer whisperer. London: Coronet.
- Schofield P(2004) Optimism and survival in lung carcinoma patients. Cancer 100 (6) 1276–82.
- Schulz R (1996) Pessimism, age, and cancer mortality. Psychol Aging. 11, 304–309.
- Shahidi J (2010) Not telling the truth: circumstances leading to concealment of diagnosis and prognosis from cancer patients. European Journal of Cancer Care 19, 589–593.
- Turner KA (2014). Spontaneous/radical remission of cancer: Transpersonal results from a grounded theory study. International Journal of Transpersonal Studies 33 (1) 42–56.
- You Me Big C Podcast (2018–2019) Available at: www.bbc.co.uk/ programmes/p0608649/episodes/downloads (accessed 2 June 2019).






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}