

Self-compassion and resilience for health- care professional
Kai Krüger, Rites of passage guide; educational trainer, Faculty of Family Medicine, University of Freiburg
Published in JHH16.2 – Faith, hope and love in healthcare
I trained as a rites of passage guide before my medical education. Consequently my perspective on its educational and professional structures recognised the importance of supporting life transitions, and viewed resilience as a key factor in sustaining people who help others. Having developed ways of supporting their self-care, I now run seminars, communication trainings and workshops on resilience for healthcare professionals.
[bctt tweet=”The approach for building resilience that I offer is specifically designed for healthcare professionals” username=”BritishHolistic”]
Introduction
More than 20 years ago my aunt, who is a pediatrician, told me she had chosen the most beautiful profession in the world. I didn’t quite understand what she meant at the time, about human connection, authenticity, love and faith as essential qualities of a doctor. But now, after training and working as both physiotherapist and doctor, I agree with her: helping and supporting others is one of the most satisfying and inspiring jobs I can imagine. Having said that, aspects of this work too often neglected or even surrounded by taboos are health professionals’ own self-care and emotional wellbeing. I certainly remember many times when giving advice to others was easier than having an honest confrontation with myself. But if you can’t help yourself, how can you help others? Though it is legitimate and important to remind others about their need for self-care, professionals suffering burn-out or addiction, mental and somatic illness, who are not enjoying life or working with others, need to discover self[1]compassion. In this article I will share my journey with you, say why I chose to address the resilience of people who study and work in healthcare, and present a framework for doing so
An analysis of need
Is building resilience actually needed for healthcare professionals? The research illustrates why we must. Rotenstein et al (2016) reported the prevalence of depressive symptoms among a total of 120,000 medical students was 27.2% overall, with some variation between different universities depending on their system of grading. Many other authors report on the prevalence of psychological illness among healthcare students. A 2015 systematic review found the rate of depression among resident physicians was 28.8% (Mata et al, 2015), and among resident surgeons Dimou (2016), who gave the prevalence of burnout at more than 50%, identified a lack of programmes for supporting them. By comparison, the estimated overall prevalence of depression in the general population is only 4.4% (WHO, 2017).
Building resilience for healthcare students and professionals
Self-compassion is a key element for building resilience. In my own experience and that of friends and colleagues, self-care was seriously lacking. I wanted to do something about this but I didn’t know how to. While one option would be to protest against the organisational factors we are facing (Balme, 2015), I chose instead to find ways of supporting individuals, and their medical community to deal better with the impact of the daily challenges faced in the healthcare system. This work took me several years and as the approach continually grows, evolves and changes it is still far from complete.
At first, the concept of resilience, though fascinating, was hard for me to grasp: easy and nice to talk about, yet difficult to create a clear concept of it. For instance, I thought at first that one simply had resilience or not. The American Psychological Association (2019) defines resilience as ‘the process of adapting well in the face of adversity, trauma, tragedy, threats or significant sources of stress’. Among its various suggested processes for building resilience are ‘making connections’, ‘looking for possibilities of self-discovery’, ‘taking care of yourself’, ‘developing realistic goals’ and ‘moving towards them’.
A resilience-building framework
The approach for building resilience that I offer is specifically designed for healthcare professionals. Depending on available time and resources, the aim of these seminars is to initiate participants – doctors, or nurses, or psychotherapists – to talk about real experiences and have them affirmed by their peers. Simply put, people gather in a safe and respectful environment, share with others what matters to them, then go out into nature to contemplate the things that they feel are important. Eventually, they come back, sit with the others again and share what has happened. The following sections introduce the foundational elements of this work.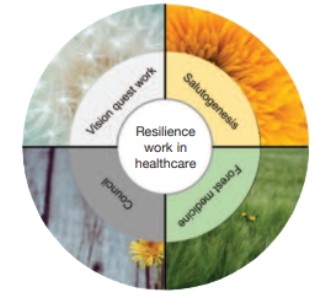
Council and its implications for modern healthcare
Council has been used in a variety of environments – seminars, schools, companies and conflict zones (Mehl[1]Madrona, 2014) – as a non-violent, non-hierarchical form of communication (Zimmerman and Coyle, 1996). It calls for authentic self-expression through active listening in a secure and stable group setting. It is unusual for professional helpers to talk about themselves, and they often need initially to overcome their discomfort with its non-directiveness, and realise that for the topic being addressed there can be no clear ‘diagnosis’ or concrete conclusion at the end. However, if a non-judgemental attitude can be maintained it offers a space for participants to express feelings on difficult issues without being judged or feeling overloaded with ‘solutions’. A wonderful example was a physiotherapy student who sang a child[1]hood song, a fond memory of a time before his parents divorced. The voice was clear and strong, and tears were flowing. Group experiences such as these are an important encounter with authentic communication and self-compassion. Although right after the council session, other participants tried to ‘help’ that person, the one singing got to experience their feeling and have them witnessed without others trying to ‘fix’ them or offer ‘solutions’.
The university programmes offered at the Hogeschool van Amsterdam and the University of Freiburg, described below, provide an excellent framework for experiencing compassion and interconnectedness.
Forest medicine and its implications for modern healthcare
Historically, in difficult times human beings have sought solace by re-connecting to the natural world. This experience may have in it elements of consolation and atonement – with oneself and with the surroundings. In recent years, as researchers confirm the benefits of time spent in forests on physical (Lee et al, 2017; Li and Kawada; 2011, Ochai et al, 2015) and mental health (Ochiai et al, 2015, Li and Kawada, 2011), western medicine is finding a rational framework for being in nature and even of measuring its effects. Having these basic human elements supported by research and academic institutions is a wonderful trend and I hope it will grow and consolidate.
Rites of passage work and its implications for modern healthcare
Rites of passage work is a field put forward in western cultures by Foster and Little in the 1970s (Foster and Little, Self-compassion and resilience for healthcare professionals SELF-COMPASSION The dandelion: a powerful image of resilience Resilience work in healthcare Figure 1:The four aspects for fostering resilience in healthcare 16 © Journal of holistic healthcare ● Volume 16 Issue 2 Summer 2019 1994). Using anthropological methods they looked at various indigenous ceremonies and social systems with the question of how these societies enable their youths to become responsible adults who can play a full part in a well-functioning society. Supported by the works on rites of passage of van Gennep (2013) and Joseph Campbell (2004) on mythology, they hypothesised common and core elements for transitioning into adulthood: initiation, separation and return. These three phases, essentially, are what Joseph Campbell coined as ‘the monomyth’ (Campbell, 2004).
Medical training is long and demanding, and as a consequence of my own training I came to inhabit a very specific role. Subsequently I have arrived at an under[1]standing of how this role has arisen and why it has now become part of me. As a rites of passage guide, I perceive the medical training as a time of transition, almost like a journey into a new life, during which the role of ‘healer’ gets modelled by training and shaped by role models, both positive and negative. This is the resource one draws on as the heavy responsibility of a doctor’s work is conferred at graduation. At a German medical graduation ceremony there are speeches, drinks and food, and in my case reflections on how well the students have performed compared with other universities, mainly with the aim of showing the university in a good light. Probably, the ceremony is more important for parents than it is for graduates. And so it might be reasonable to assume that this ceremonial confirmation of medical training has nothing in it of the initiatory experience such a momentous transition actually requires. If so, medical education, lacking such a crucial right of passage, turns healthcare professionals out into their adult profession incompletely initiated
Reflections on implementing resilience programmes
Our program KoSeiM – Kommunikation and Selbsterfahrung in der Medizin (translating as communication and self-discovery in medicine) at the University of Freiburg has been presented at the German conference for medical education (Krüger, 2015). In this optional course, 10 students met for three sessions of three hours to share and reflect on their positive and negative experiences of medical education. The work included identifying positive role models and exploring coping strategies for the many challenges they experienced, and sometimes critical discussion. The participants had a constant struggle with the feeling that ‘in the time I am sitting here I could study another three hours for another exam’. Having said that, during the same communication training some students opened up about a suicide in their community. For some, it was the first time this loss had been addressed and the support from the group was perceived as helpful and soothing. Resilience programmes have been implemented for physiotherapy students at the Hogeschool van Amsterdam, and for medical students at the University of Freiburg in several, semester-long formats. The course was supported and organised by the department of family medicine of the University of Freiburg free of charge, yet in my experience, offering resilience building programmes meant we received a lot of hesitant looks, sly jokes and resistance from people working in healthcare. Most obvious are the organisational challenges of finding curriculum time and financial backing. Moreover the medical community needs a narrative – in language and symbol – that can open up the self-care space to medical students as a requirement for sustaining wellbeing, health, good practice and a long career. In my experience the language has to be very clear and academic, and the possibility of obtaining a certificate at the end of a course seems to raise the acceptance among the student community. On the other hand words that sound ‘touchy-feely’ will act as a deterrent. I well remember an incident at the Hogeschool van Amsterdam, where the comment to ‘speak from the heart’ resulted in a massive disapproval of the suggested council-style element.
In summary, the process of implementation needs time and patience, reciprocal support and persistence from the people who promote it. Nevertheless resistance will be faced, sometimes overcome, and sometimes not.
Perspectives and outlook
Despite the obstacles I will continue to promote resilience as an important resource and necessary competence for healthcare professionals. For the present our seminars are privately funded. This year though, for the first time, I was invited to speak about resilience at a conference on integrative medicine for medical students in Germany at the University of Witten/Herdecke’s summer school. The recognition of widespread burnout and the demographic shifts and chronic diseases proliferating requiring more biopsychosocial approaches is driving changes in the content of medical training. Medical curriculae are now widely under review, and this potential for reformation, will, I believe, include a far greater emphasis on the resilience of patients and their doctors. Yet there is much to do before the vision, inspired by my aunt, of a medical community for whom being a doctor is ‘the most beautiful job in the world’. In achieving this the essential qualities of human connection, authenticity, love and faith remain for me important and central.
References
- American Psychological Association (2019) The road to resilience. Available at: www.apa.org/helpcenter/road-resilience (accessed 11 May 2019).
- Balme E (2015). Doctors need to be supported, not trained in resilience. BMJ 351.
- Campbell J (2004) The hero with a thousand faces: commemorative edition. Bollingen series. Princeton, NJ: Princeton University Press.
- Dimou FM, Eckelbarger D, Riall, TS (2016) Surgeon burnout: a systematic review. Journal of the American College of Surgeons 222, 1230–1239.
- Foster S, Meredith L (1994) Vision quest: Sinnsuche und Selbstheilung in der Wildnis. Munich: Goldmann.
- Krüger K, Lim D (2017) KoSeiM – Kommunikation und Selbsterfahrung in der Medizin. In: Gemeinsame Jahrestagung der
- Gesellschaft für Medizinische Ausbildung (GMA) und des Arbeitskreises zur Weiterentwicklung der Lehre in der Zahnmedizin (AKWLZ). Düsseldorf: German Medical Science GMS Publishing House.
- Lee I, Choi H, Bang K.-S, Kim S, Song M, Lee B (2017) Effects of forest therapy on depressive symptoms among adults: a systematic review. International Journal of Environmental Research and Public Health 14, 321.
- Lee J, Tsunetsugu Y, Takayama N, Park B-J, Li Q, Song C, Komatsu M, Ikei H, Tyrväinen L, Kagawa T, Miyazaki Y (2014) Influence of forest therapy on cardiovascular relaxation in young adults. [Online]. Evidence-Based Complementary and Alternative Medicine. https://doi.org/10.1155/2014/834360
- Li Q, Kawada T (2011) Effect of forest therapy on the human psycho-neuro-endocrino-immune network. Nihon Eiseigaku Zasshi 66, 645–650.
- Mata DA, Ramos MA, Bansal N, et al (2015) Prevalence of depression and depressive symptoms among resident physicians: a systematic review and meta-analysis. JAMA 314 (22) 2373–2383.
- Mehl-Madrona L, Mainguy B (2014) Introducing healing circles and talking circles into primary care. Perm J 18, 4–9.
- Ochiai H, Ikei H, Song C, Kobayashi M, Miura T, Kagawa T, Li Q, Kumeda S, Imai M, Miyazaki Y (2015a) Physiological and psychological effects of a forest therapy program on middle-aged females. International Journal of Environmental Research and Public Health 12, 15222–15232.
- Ochiai H, Ikei H, Song C, Kobayashi M, Miura T, Kagawa T, Li Q, Kumeda S, Imai M, Miyazaki Y (2015b) Physiological and psychological effects of forest therapy on middle-aged males with high-normal blood pressure. International Journal of Environmental Research and Public Health 12, 2532–2542.
- Rotenstein LS, Ramos MA, Torre M, Segal JB, Peluso MJ, Guille C, Sen S, Mata DA (2016) Prevalence of depression, depressive symptoms, and suicidal ideation among medical students. JAMA 316, 2214–2236.
- Van Gennep A (2013) The rites of passage. London: Routledge.
- WHO (2017) Depression and other common mental disorders: global health estimates. Geneva: World Health Organization. Zimmerman JM, Coyle V (1996) The way of council. Vol 2. Las Vegas, NV: Bramble Books






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}