

Holistic approach to improve community health – The AYUSH approach
S Manasi, Associate Professor, Centre for Research in Urban Affairs, Institute for Social and Economic Change, Bangalore
KV Raju, Assistant Director and Principal Scientist, International Crops Research Institute for Semi Arid Tropics, Patancheru, Telangana
Published in JHH12.2 – Works that reconnect
Since my childhood I have taken simple home remedies for minor ailments. Hence, I am always inclined towards healing processes that are close to nature.When I visited an ayurvedic doctor as a child, I was given a one page note indicating the ‘dos and don’ts’ for good health and wellbeing. Interestingly apart from the physical aspects of healthcare, the list contained points on emotional health indicating conscious living by curtailing emotions like anger, hatred, jealousy, and to keep calm, meditate and so on. Although it did not register much in my mind, then, I realise that it indicated stress management principles. So, introduction to holistic health is part of growing up in India. But this is dying wisdom and providing healthcare access in India is a challenge with exorbitant costs affecting millions, particularly the poor.
S Manasi
Experiences of simple healing methods, yoga, and preventive health care practices have always appealed to me. Erroneous practices of healthcare, wrong food habits, and sedentary lifestyle have overridden simple remedies, placing a huge burden on our economy and affecting quality of life. I have been one of the members of the core committee of the AYUSH programme initiative at the state government and was keen to see if the intervention was transforming people’s lives locally and appealed to the community at large.The study certainly motivated me, showing that interventions would work well at the ground level if the right approaches were adopted.
KV Raju
Introduction
Healthcare is the right of every individual but in India the lack of infrastructure and qualified professionals, as well as poor access to basic medicines and facilities, thwarts its reach to about 60% of the population. (Vyasulu and Vijayalakshmi 2003). The health status of Indian people and the healthcare services available to them are issues of great concern (Peters et al 2002). Government spending on primary healthcare is being wasted due to improper planning, financing and organisation of its delivery system (Duggal 2000). India spends 4.2% of its gross domestic product on healthcare, the bulk of which represents private out-of-pocket expenditure. Among urban households, 70% of all visits made are to private sector providers, and the remaining 30% are evenly divided among the public primary healthcare centres and hospitals (Das et al 2012). Given this backdrop, traditional systems of medicine can be a good alternative to promote healthcare in rural settings.
Traditional medicine is a synthesis of therapeutic experiences from generations of practising physicians of indigenous medical systems (Deb 2012). Although traditional systems of medicine have been around for thousands of years, no integration exists between them and allopathic medicine. With the growing need for safer drugs, a greater attention has been drawn to the quality, efficacy and standards of the traditional Indian medicine formulations (Ravishankar and Shukla 2007).
India has a rich heritage of traditional medicine with these modes of healthcare flourishing through many centuries. Medicinal plant-based systems are playing an important role in providing healthcare to a large section of the population, especially in the developing world (Ravishankar and Shukla 2007). ‘Indian systems of medicine’ include both those which are considered to be of Indian origin and others which have come to India from outside and been assimilated into Indian culture (Prasad 2002). The Indian healthcare system has recognised six such systems in this group – ayurveda, siddha, unani, yoga, naturopathy and homoeopathy (Rajeev 2012). The WHO has taken a keen interest in this, realising the role of traditional and alternative systems of medicine in the health sectors of both developing and developed countries. This issue has been globally addressed through the traditional medicine programme of the WHO via several routes ranging from the cultivation of herbs, manufacturing and dispensing to the preparation of guidelines for common illnesses (like cold, cough, headache, fever) in traditional systems of medicine.
The Department of Ayurveda, Yoga and Naturopathy, Unani, Siddha and Homoeopathy (AYUSH), Central Council of Research in Ayurveda and Siddha, and numerous other collaborative centres of the WHO in India are assigned with appraisal project work and direct financial cooperation projects that are aimed at strengthening the programme.
AYUSH (ayurveda, yoga & naturopathy, unani, siddha, homeopathy)
The Department of AYUSH was created as the Department of Indian System of Medicine and Homeopathy in 1995 and re-named the Department of Ayurveda, Yoga & Naturopathy, Unani, Siddha and and Homoeopathy (AYUSH) in 2003. It focuses on development of education and research in AYUSH systems and was elevated to an independent ministry in 2014. It promotes the model of AYUSH grama panchayat where AYUSH healthcare facilities including hospitals are set up in one village to serve a group of villages. The AYUSH grama panchayat project in Karnataka is a government sponsored public-private partnership programme. It is a unique project which is designed to bring cost-effective and affordable healthcare to the general public as part of promoting a holistic approach to improving lifestyle change.
The overall health check of the entire population is done by AYUSH doctors based on AYUSH systems. The communities are educated in healthy practices and the advantages of traditional food items used locally including their medicinal properties. AYUSH doctors also run health check-up camps at schools and in selected villages and train others to promote various health programmes. These include accredited social health activists (ASHAs – community health workers), anganwadi (government sponsored mother and childcare centres) workers, and teachers; awareness building activities are also conducted through grama panchayats (village councils) involving schools, anganwadis, self-help groups and other community organisations.
Objectives of AYUSH grama panchayat
Specific objectives include the enhancement of health indicators, avoidance of diseases, promotion of healthy lifestyles, training in preparation of home remedies for common ailments, promotion of yoga, meditation and nature cure, conducting specialised therapies, prevention of communicable/non-communicable diseases/local endemic diseases, research and training for capacity building
Soukya Foundation’s intervention through AYUSH grama panchayat
The Soukya Foundation (SF) Charitable Trust was established in Bangalore in 1996 to extend free quality treatment to local people. Against this backdrop, the government of Karnataka, with the support of Department of AYUSH, Department of Health and Family Welfare and SF, established a rural healthcare centre in Jadigenahalli in Bangalore rural district. This centre (known as Dr Mathai’s Rural Holistic Medical Centre – DMRC, SF) is the first of its kind with an integrated holistic treatment approach to improving community healthcare.
Our study aimed to:
- understand and analyse the impact of the DMRC, SF on improving rural public health
- identify key challenges in improving public health in the context of the AYUSH programme
- provide a way forward for a sustainable holistic model integrating protection of health and ecology.
Data sets from the DMRC, SF and primary data from households using a structured questionnaire covering socio-economic aspects, AYUSH activities, preferences and perceptions of healthcare centres, access to healthcare, user satisfaction, sanitation, ecology and cultural aspects were analysed. Responses were collected from a total of 102 households (10% of the sample) across five villages for the survey.
Healthcare activities include ayurveda, yoga, naturopathy and homeopathy. Based on the patient’s response to reatment, this might consist of (a) homeopathy; (b) homeopathy and ayurveda;
(c) homeopathy, ayurveda and yoga; (d) homeopathy, ayurveda, naturopathy, yoga.
Healthcare activities
- Panchakarma therapy – panchakarma is a therapeutic way of eliminating toxic elements from the body according to ayurveda. These treatments are not free but are reduced by 20%.
- Balopachara (paediatric care) – balopachara is a homeopathic treatment for children under 12 years aimed at helping increase immunity and building resistance to diseases. They are also given nutritional supplements. 586 children have been treated so far.
- Mother and child care – this programme mainly focuses on maternal health and neonatal care of infants. The expectant mothers are given ayurveda medicines and are checked for physiological changes, encouraged to exercise, made aware of natural birthing, listen to music, and educated about healthy food habits for healthy pregnancy. In addition, women are taught pranayama (breathing exercises) and sukshayama (finger loosening, eye and head exercises) for promoting normal delivery.
- Prevention of viral diseases – the AYUSH approach towards prevention of viral diseases is holistic and works on prevention of diseases through homoeopathic preventive medicine for ailments like dengue and chikungunya. Training builds awareness about cleanliness and personal hygiene and shows how to make natural mosquito repellents from locally available plants such as neem/marigold. About 190 homes covering 760 people have been given preventive homeopathy medicine.
- Vector-borne disease – this programme covers awareness about types of vector-borne diseases; incubation period; manifestation of diseases; complication of diseases; measures to control the disease; cultivation of medicinal plants like marigold, eucalyptus, tulsi etc around houses to prevent mosquitoes.Training is given in preparing homemade repellents using home ingredients like bajee, vidanga, camphor, sambharani powder, gomuthra, arka.
- De-addiction promotion programmes – AYUSH grama panchayat runs awareness-raising programmes and provides homeopathic medicines. Some are treated in the hospital while others are treated by doctors through personal visits and persuasion.
- Geriatric care – this provides treatment to the elderly population beyond 60 years of age. This programme has been recently introduced and so far 393 patients have been treated.
- Yoga therapy programmes – are conducted regularly every day across villages and various locations to spread the message of yoga to help various ailments. So, far, 466 yoga therapy programmes have been held.
- Home remedies programme – home remedy treatments are aims at curing diseases/ailments with commonly available spices, vegetables, herbs or other plants. DMRC, SF’s role has been to educate people on these lines to prevent minor illnesses at affordable costs and reduce medical costs. DMRC, SF, works through ASHA workers and individual training programmes for local people.
- Herbal and kitchen gardens – 215 people have taken part in this well-received programme.
Educational activities
Yoga
Yoga classes are part of the curriculum in schools and were compulsory before DMRC, SF’s initiation. However, yoga classes conducted by DMRC, SF have reinforced and strengthened the programme. 119 students egularly take part.
Health and hygiene
SF promotes health and hygiene practices to children in all schools – keeping their environment clean and maintaining personal hygiene such as regular hand washing, oral hygiene etc.
Checkups at anganwadis
SF has focused on preventing mortality among children through conducting monthly check-up programmes in anganwadi centres. Children are checked for malnutrition, physical growth, haemoglobin levels and respiratory ailments. Later, children diagnosed with ailments are provided ayurveda/homeopathy medication and monitored regularly. 163 children have been provided treatment.
Processes: Awareness creation programmes
DMRC, SF has adopted different approaches towards creating awareness about its activities and their purpose. Announcements, distribution of pamphlets and banners were used. Besides this, it conducts free monthly medical camps to screen patients for diabetes, hypertension, haemoglobin count and other ailments, besides prescribing medication. Awareness creation has helped spread positive effects in terms of people accessing treatment at DMRC, SF, telling neighbours about the services and sharing their experiences. Overall, 67% of people have influenced others, 41% have influences their own family members, and 16% have relatives who travelled from neighbouring villages for treatment at DMRC, SF
Key Findings
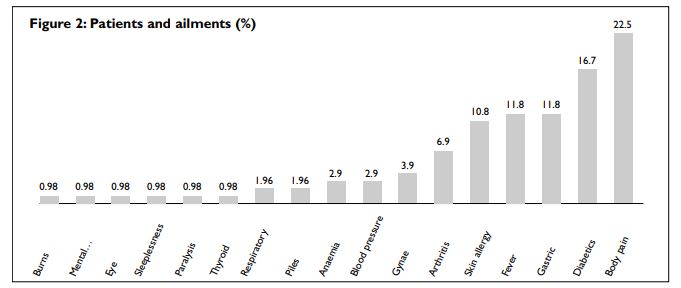
This section captures people’s perceptions regarding healthcare treatments, educational programmes and other activities provided by DMRC, SF. The doctors in DMRC, SF are unique in their diagnosis and treatment methods. They initially identify the root cause of a given disease through laboratory tests/scans. They go about treatment differently to the approach of the private clinics (see Figure 1).
Overall perception regarding treatment
People responded positively about the approach of doctors in listening to patients’ ailments and recording details. Patients are generally attracted by free check-ups done for diabetes/hypertension with free medicines provided. Several patients have been able to see improvements in their health status with changes in lifestyle combined with medication.
Treatment for different ailments
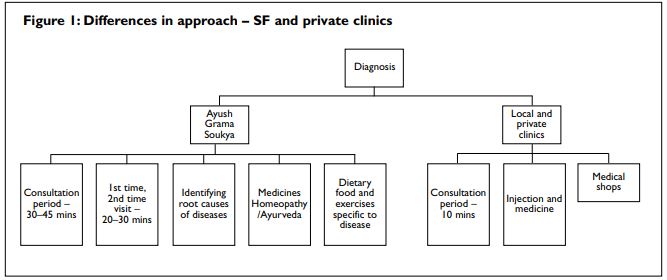
The most common reason for patients visiting DMRC, SF is body pain (22.5%), followed by diabetics (16.7%) fever (11.8%) and gastric ailments (11.8%). The doctors observe that villagers are more prone to body pain because of physical work. Gastric and weakness problems are due to irregular food intake. Changes in lifestyle and food habits among rural people have led to chronic diseases like diabetes (16.7%), hypertension (2.9%) and respiratory problems (1.96%) (see Figure 2).
Patients’ preferences
Jadigenahalli has three private medical clinics and one primary healthcare centre (PHC). Patients generally visit one of these clinics for treatment. Patients from low income groups largely visit private clinics, PHC, and government hospitals located in Hoskote or Malur (12 kms away) while patients belonging to high income groups travel to private hospitals in Hoskote. With DMRC, SF being close to the PHC, several patients tend to visit it as an alternative. Treatment at private clinics at Jadigenahalli place a cost burden on the poor and DMRC, SF’s intervention is considered a welcome initiative.
Priority for diabetes and hypertension
Diabetes and hypertension are the two most common ailments observed. Previously 8.8% of BP and 13.73% of diabetic mellitus patients preferred Hoskote and private clinics in Jadigenahalli. However, after intervention by SF, 5.88% BP and 11.7% of diabetic patients have chosen DMRC, SF for treatment. These changes indicate that people are trying DMRC, SF’s treatment. This could be attributed to the time spent with the patients, awarenessraising programmes and positive impacts experience.
Patients’ interest in visiting DMRC, SF
Patients who are visiting SF on a regular basis, with ongoing follow-ups, vary from 26% in the past six months, 23% once in a month and 5% once year. Within a short period, DMRC, SF has been able to draw attention of the villagers through its holistic and traditional approach of medicines and treatment. However, follow-up visits by some patients due to busy schedules and negligence continues to be an issue.
Benefits of yoga
Yoga is a welcome initiative bringing about considerable changes among the people in the villages. Children experience benefits with respect to their health, influencing their lifestyle and food habits and this improvement in children’s health has attracted the older population.
Challenges
- Getting doctors to stay in villages.
- Providing free services and maintaining funds in the long run.
- Influencing implementation of lifestyle change and dietary habits among diabetic patients.
- Hygiene and changes in habits take time and are difficult to influence.
- Approaching people to enrol for de-addiction programmes is challenging.
Towards a sustainable approach
The current model of health care followed by DMRC, SF needs to be sustainable in the long run and replicated socially, economically and environmentally.
Financially sustainable options
Possible financial options could vary charges for different economic groups – free medicines, a small fee or the standard amount. Donations from other institutions could be of some help. The government could think of continuing the support for a longer period until the programme can be sustained on its own.
Strengthening institutions and integration
The DMRC, SF is a public-private venture with the main motto being to build the good health status of the rural people; the government of Karnataka, under the AYUSH grama panchayat central scheme, provides Rs.34.95 lakh (£35,369) and three acres of land for the programme. There is scope for involving other formal and informal institutions at local and regional levels to work on various dimensions and so strengthen the programme by complementing each other.
Networking for outreach
There is a scope for NGOs, organisations through corporate social responsibility (CSR), religious institutions, educational institutions, philanthropists, research institutes or similar organisations to contribute to this programme carrying out continuous research and learning. There could be streamlined programmes focusing on sanitation and hygiene, and educational programmes for students at various levels could be explored.
Involving self-help groups and youth organisations
Jadigenahalli has around 46 self-help groups (village based financial intermediaries with10 to 20 members. Members make small regular savings contributions over a few months until there is enough capital in the group to begin lending). All members of self-help groups are aware of DMRC, SF, and its activities and see the initiative as positive. There are two youth organisations (private non profit organisations dedicated to helping emotionally and behaviourally troubled villagers and their families) willing to work with DMRC, SF.
Strengthening personnel’s communication skills
ASHA workers engaged by DMRC, SF have basic high school or pre-university education. A major role of ASHA workers is to motivate people about AYUSH and to get treatment at DMRC, SF by strengthening the relationship between DMRC, SF and the local population. ASHA workers express the need for further training in persuasion skills, communication skills, handling varied situations etc. Besides these soft skills, some basic knowledge about diseases/growing herbal plants/home remedies would also be useful.
Influencing people on lifestyle change and holistic treatments
People in general are more used to allopathy medicines and because of easy access to medicines at medical shops/ local shops (eg painkillers), self-medication is common. As painkillers provide an immediate relief, people depend on them. Lifestyle changes mean they have to make efforts in terms of giving up on various things and practising yoga which may not be convenient; time constraints are seen as an easy excuse. Urban lifestyle largely influences people to approach private hospitals and those who enjoy a better economic status are more likely to visit private hospitals.
Protection and conservation of ecology
Water protection and conservation measures
Jadigenahalli is in a semi-arid zone with a severe water scarcity. It is important to work on short-term and longterm solutions while addressing this issue to ensure the sustainability of other programmes. Rainwater harvesting needs to be promoted.
Need to promote organic farming
Many farmers use fertilisers and pesticides without protection. Discussions with farmers reveal that they are fairly aware of the negative impacts but are negligent in protecting themselves. Concerns regarding the changing scenario of agriculture system, uncontrolled use of fertilisers, depleting groundwater levels and the effect for health and environment are serious. Hence, some village leaders are keen for training in organic farming and awareness about fertiliser/pesticide effects on health.
Need for improved sanitation
Awareness programmes on health and hygiene need to be promoted. Toilets construction is largely covered but there is still some open defecation which could be curtailed. Besides this issue, a greater concern relates to solid waste management. Garbage is widely strewn, resulting in poor hygiene. There is a need for streamlining garbage management.
Conclusion
Healthcare is the right of every individual but lack of quality infrastructure, dearth of qualified medical professionals, and poor access to basic medicines and medical facilities means 60% of the population are not covered. The challenge of providing rural healthcare in India, with costs and infrastructure challenges on the rise, sees a traditional holistic medicine approach as a positive option for improving the health of the masses. The SF project has had a positive impact for economically poor communities.
This article is based on Ecology, climate change and coping mechanisms for health and livelihoods in semi arid tropics of India – a case study of Jadigenahalli Grama Panchayat in Karnataka undertaken by the Centre for Ecological Economics and Natural Resources, Institute for Social and Economic Change, Bangalore and Centre for Research in Urban Affairs funded by ISEC. Other team members included Hemalatha BR, Poornima S and Rashmi KP
References
- Das J, Holla A, Das V, Mohanan M, Tabak D and Chan B (2012) In urban and rural India, a standardized patient study showed low levels of provider training and huge quality gaps. Health Affairs 31 (2).
- Deb R (2012) Prospects, problems and approaches to alternative system of medicine: a review. International Journal of Ayurvedic and Herbal Medicine 2(1) pp 192–197.
- Duggal R (2000) The private health sector in India – nature, trends, and critique. New Delhi: Voluntary Health Association of India.
- Peters D, Yazbeck A, Sharma R, Ramana GNV, Prichett LH, and Wagstaff A. Better health systems for India’s poor – findings, analysis and options. Wasthington DC: World Bank.
- Prasa LV (2002). Indian system of medicine and homoeopathy traditional medicine in Asia. Ranjit Roy Chaudhury and Uton Muchatar Rafei Eds. WHO-Regional Office for South East Asia – New Delhi. pp283–286.
- Ravishankar and Shukla (2007) Indian systems of medicine: a brief profile. African Journal of Traditional, Complementary and Alternative Medicines 4 (3) pp 319–337.
- Vyasulu P and Vijayalakshmi V (2005) Reproductive health services and role of panchayat in Karnataka. Paper presented at the seminar on Development in KarnatakaA Multi Disciplinary Perspective, June 10–12th 2005, Institute for Social and Economic Change and Cornell University
- World Bank (1995) India: policy and finance strategies for strengthening primary health care services. Washington, DC: World Bank.
- Yadav V, Jayalakshmi S, Rajeev KS (2012) Traditional systems of medicine – now and forever. Central Pharmaceutical Sciences 3 (4).






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}