

How can holistic healthcare influence health inequalities?
Deeya Kotecha, Final year medical student, University of Cambridge
Published in JHH 18.3-Shifting the paradigm
I have learnt a lot of things in the last few years of medical school, but the importance of health inequalities and health inequities was not one of them. As future doctors, we spend a lot of time learning about the drugs and interventions to treat different conditions but very little time on addressing the wider determinants of health.
Without an unexpected foray into global health, followed by an almost obsessive devouring of books like The Health Gap (Marmot, 2015) and The Spirit Level (Pickett & Wilkinson, 2010) I doubt I would have truly understood the importance of holistic care and public health within medicine. Indeed, if had you asked me what the most important determinants of health were, I would have rattled off a conventional list: smoking, alcohol, obesity, diet. However, other holistic aspects, for example poverty or loneliness, are also significant and without a full consideration of these we can never expect to address health inequalities.
To illustrate the importance of holistic healthcare I shall use an example case of Betty, a 47-year-old woman, from Rochdale.
At first glance, it can be tempting to take an elementary approach. Betty has COPD because she is a long-term smoker, and her diabetes and hypertension are probably a combination of her physical inactivity, high-salt, high-fat diet, and smoking. If we could encourage her to become more active, lose some weight and quit smoking, her health would significantly improve. She also has depression. According to the National Institute of Health and Care Excellence, we should assess her and depending on severity offer an anti-depressant, cognitive behavioural therapy (CBT) or both (NICE, 2012). It is without doubt that if successfully implemented these factors would help. However, does this really address the crux of the problem? Conveying advice alone is highly unlikely to help. Betty knows that her diet and smoking are unhealthy and so ignorance is not the problem. Instead, it is that she does not feel able to make healthy choices and to understand this we need to consider her life and the community in which she lives.
Rochdale, where Betty lives, is the 15th most deprived borough in England with a crime deprivation domain which is the second worst in the entire country. While there are green spaces, these often become dangerous at night, meaning even if Betty wanted to exercise after work, she could not. Betty does not have a car, and instead does her weekly shop from her local grocery store, supplemented by meals from the four, cheaply priced, fast-food takeaways on her road.
When Betty comes home from work, she is tired; she does not earn the living wage and so taking a bus to a larger supermarket is a luxury she cannot afford. Thus, given her economic constraints and surrounding environment, a sudden switch to walking 10,000 steps a day and following a Mediterranean diet, the advice regularly offered, is difficult.
‘The difference between Hackney and the West End is the same as the difference between England and Guatemala in terms of life expectancy’
Poverty is an essential component of health, accounting for the social gradient which exists. A famous representation of this was demonstrated on the Jubilee tube line in London with each stop from Westminster leading to a drop in life expectancy of one year (Dangerfield, 2012). Indeed, the difference between Hackney and the West End is the same as the difference between England and Guatemala in terms of life expectancy (Marmot, 2012).
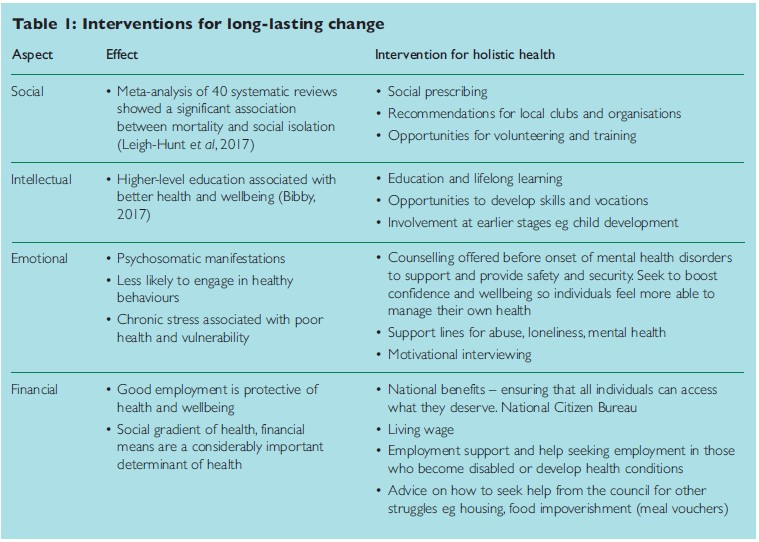
But why is this, and what is the cause? Poverty leads to patients using less preventative healthcare, being less attentive to their health and failing to adhere to drug treatments, even when costs are covered. One theory is that scarcity narrows a person’s working memory leading to reduced forward planning and sense of control (Marmot, 2015). Working with Betty to improve her financial situation, be that through the council or employment support interventions would undoubtedly place her in a better position to look after health. Indeed, looking beyond the medical causes, and more at the causes of the causes, is the only way to inspire long-lasting change. Other ways to address this are summarised in Table 1.
Let’s take this one step further and consider Betty’s social and emotional wellbeing.
 Offering CBT or anti-depressants may treat her depression, but it will not address the underlying causes, which will probably culminate to affect another aspect of Betty’s health in the future. Instead, using a holistic approach would involve using a broad range of resources from statutory and voluntary services. This could include social prescribing, motivational interviewing to incorporate changes to Betty’s routine and tailored counselling to enable Betty to understand her depression and loneliness. Social prescribing could facilitate access to local community services and activities such as craft groups, adult learning or leisure facilities, solidifying Betty’s social engagement.
Offering CBT or anti-depressants may treat her depression, but it will not address the underlying causes, which will probably culminate to affect another aspect of Betty’s health in the future. Instead, using a holistic approach would involve using a broad range of resources from statutory and voluntary services. This could include social prescribing, motivational interviewing to incorporate changes to Betty’s routine and tailored counselling to enable Betty to understand her depression and loneliness. Social prescribing could facilitate access to local community services and activities such as craft groups, adult learning or leisure facilities, solidifying Betty’s social engagement.
‘When someone becomes sick, how can we treat the illness and then send them back to the very conditions which made them sick in the first place?’
An example of such a successful intervention is the Hackney WellFamily Service which provides short-term counselling, advice and practical support for adults. It uses holistic interventions to address financial status, social networks, and education. 81% of those who used the service felt that it had helped them to achieve their goals and 99% rated it as good or excellent.
‘Taking a holistic approach and working to address the causes of the causes undoubtedly helps to reduce health inequalities’
Taking a holistic approach and working to address the causes of the causes undoubtedly helps to reduce health inequalities. However, it is also important to remember that social determinants act at every stage in a person’s life: from cradle to grave, and we should be acting at every point to lessen inequities (Marmot, 2017). In the case of Betty, addressing her issues earlier from a holistic approach could have created a preventative effect, lessening the disease burden and disparities that exist between her and those most privileged.
Conclusion
The conditions in which we live our lives are what affect our health. Unfortunately, the quality of these conditions is not equally distributed and thus we cannot expect health to be either. When someone becomes sick, how can we treat the illness and then send them back to the very conditions which made them sick in the first place? To inspire change, we need to address the causes of causes and the only way to do this is holistically.
Resources
Bibby J (2017) How do our education and skills influence our health? (accessed 31 July 2021).
Dangerfield A (2012) Tube map used to plot Londoners’ life expectancy. BBC news, July 20. Accessed 29th July 2021 (accessed 31 July 2021).
Leigh-Hunt N, Bagguley D, Bash K, Turner V, Turnbull S, Valtorta N & Caan W (2017) An overview of systematic reviews on the public health consequences of social isolation and loneliness. Public Health, 152, 157–171.
Marmot M (2017) Commentary: Social determinants and the health gap: creating a social movement. International Journal of Epidemiology, 46( 4), 1335–1339.
Marmot M (2015) The health gap: The challenge of an unequal world. Bloomsbury Press.
NICE (2012) Assessment and treatment of depression in adults in primary care. (accessed 5 October 2021).
Pickett K & Wilkinson R (2010) The spirit level. Why equality is better for everyone, Bloomsbury Press.






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}