

Breast cancer screening
AntoniaWrigley GP; JHH editorial board member
Published in JHH14.2 – Women’s Health
As an NHS GP I have been following the overdiagnosis movement over the last few years. I also have a growing (and somewhat conflicting) interest in lifestyle and functional medicine. Having recently finished my GP training I am well versed in evidence based medicine and informed choice, both of which are noble ideals that I agree with in principle. In practice, however, it can be extremely difficult to deliver. On the one hand the ‘evidence’ is far from robust, and on the other not all patients have the resources or motivation to take control of their own health and make what can be complex decisions.
The central idea of early disease detection and treatment is essentially simple. However, the path to its successful achievement (on the one hand, bringing to treatment those with previously undetected disease, and, on the other, avoiding harm to those persons not in need of treatment) is far from simple though sometimes it may appear deceptively easy.
Andermann et al (2008)
Introduction
Screening makes sense to health professionals and patients/laypeople alike. It intuitively feels like a good thing to do. If we catch something early we should be able to fix it before it causes problems. It saves lives, which is surely worth the minimal harms and the cost. Well yes; but only if it is a truly effective screening test and appropriately used.
A perfect screening test would positively identify everyone who has early disease, without falsely identifying anyone who is unlikely to get the disease. But identifying this precise group is only going to be worth the effort if there are treatments available which are more effective in the early stages of the disease than they would be later on. Also, the test itself should not cause any harm.
These issues not only make decisions about screening far from straightforward, but also ensure that evaluating screening programmes will be difficult.
Synthesis of emerging screening criteria proposed over the past 40 years
- The screening programme should respond to a recognised need.
- The objectives of screening should be defined at the outset.
- There should be a defined target population.
- There should be scientific evidence of screening programme effectiveness.
- The programme should integrate education, testing, clinical services and programme management.
- There should be quality assurance, with mechanisms to minimise potential risks of screening.
- The programme should ensure informed choice, confidentiality and respect for autonomy.
- The programme should promote equity and access to screening for the entire target population.
- Programme evaluation should be planned from the outset.
- The overall benefits of screening should outweigh the harm.
(Andermann et al 2008)
The complications of diagnosis
False positives
False positive results identify people as having the disease when actually they don’t. Unnecessary further investigation, treatment and worry will inevitably follow.
False negatives
False negatives are screening results that fail to pick up people who do have the disease. This may delay a proper clinical diagnosis as the patient, wrongly reassured may not seek medical advice when subsequently she notices warning symptoms.
Overdiagnosis
Overdiagnosis occurs when doctors diagnose and treat people with early disease that would have resolved naturally or never caused a significant problem. Overdiagnosis leads to unnecessary treatment and causes needless concern for the people it labels. It will also, by including in its number well people, make a screening programme look more effective than it really is.
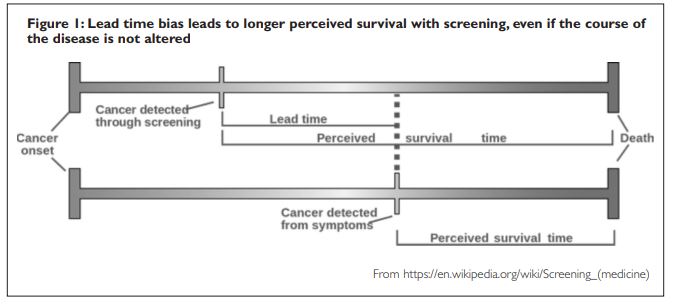
Lead time bias
As you can see in Figure 1, in a typical example of the natural history of cancer, the length of time between the onset of the cancer and death are the same. However, because screening in this case makes the diagnosis earlier the survival time seems to be longer.
Selection bias
People who perceive themselves to be at higher risk are more likely to seek screening. This selection bias could go either way but on the whole if screening attracts the ‘worried well’, or people who look after their health, the direction of the bias will tend to make screening look more effective than it is.
Publication bias
Publication bias is the result of more positive trials being submitted to journals for publication than negative trials. This may or may not be deliberate.
Mammography breast screening
Mammography was first introduced in the late 1970s to those deemed to be at high risk of breast cancer. It quickly turned into a mass screening programme, which in the UK is offered every three years to all women between the ages of 50 and 70. In England this age range is being extended to 47 to 73. Mammography screening is recommended in most western countries though age ranges and screening intervals vary. Why, then, did the Swiss Medical Board, after examining the data a few years ago, recommend against mammography screening and advise that programmes should be phased out?
The leaflet NHS Breast Screening: helping you decide states ‘The NHS offers breast screening to save lives from breast cancer’ […but] ‘screening does have some risks. Some women who have screening will be diagnosed and treated for breast cancer that would never otherwise have been found, or caused them harm.’ It acknowledges that there ‘is a debate about how many lives are saved by breast screening and how many women are diagnosed with cancer that would never have become life-threatening’ (NHS, 2015). It then goes on to give ‘best estimates’ based on the Independent Breast Screening Review (Independent UK Panel on Breast Cancer Screening, 2012) which estimates that one life is ‘saved’ for every 200 women screened (every three years between the ages of 50 and 70) but that three are overdiagnosed.
However the Nordic Cochrane Centre leaflet Screening for Breast Cancer with Mammography (2008,2012) gives quite different numbers. After analysis of the trial data up to 2008 it estimated that for every 2,000 women attending screening over a 10 year period, 1 would avoid dying from breast cancer while 10 would be overdiagnosed and 200 would have a false alarm (false positive) result. In the 2012 edition it added that ‘since these trials were performed, treatment of breast cancer has improved considerably. More recent studies suggest that mammography screening may no longer be effective in reducing the risk of dying from breast cancer.’ It also explains that treatment of healthy women (ie those overdiagnosed) increases their risk of dying eg from heart disease and cancers. It concludes that it ‘no longer seems beneficial to attend for breast cancer screening’ (Nordic Cochrane Centre, 2012).
More recently the 2015 paper Benefits and Harms of Mammography presents similar numbers based on randomised trial data and more recent observational studies. The authors extrapolated data to a population of 1,000 women invited to biennial mammography screening for 20 years from the age of 50. Using 2007 UK population data they estimated two to three breast cancer deaths in this population would be prevented, but all-cause mortality would remain the same (Loberg et al, 2015).
Particular problems with mammography
Mammography involves pressing the breast between two plates to spread out the breast tissue. This pressure can cause significant pain. It can also potentially cause a cancer to rupture making spread of the cancer cells into the blood stream more likely.
Mammography also uses radiation. X-rays are well known to increase the incidence of cancer so the test itself may make a future breast cancer more likely, especially in those already at high risk.
Mammography is up to 98% sensitive in women with fatty breast tissue; however this drops as low as 48% in the very dense breast. Unfortunately high-density breast tissue is associated with a higher risk for breast cancer and more aggressive cancers. Once again we can see that this introduces a bias that makes screening look more effective than it is.
Overdiagnosis: overtreatment and harm in screening mammography
Ductal carcinoma in situ (DCIS) was a rare diagnosis before the introduction of screening but now accounts for about 20% of screen detected breast cancers. Its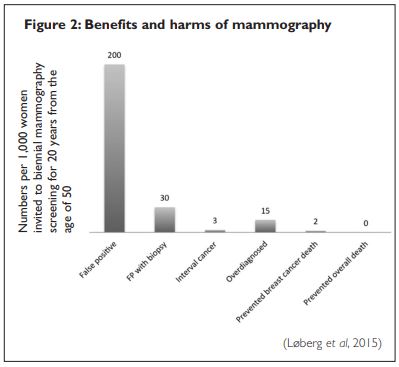 natural history is still poorly understood with many never becoming invasive cancer, yet 30% of DCIS is treated with mastectomy. The charge of overdiagnosis of DCIS is selfevident. However there is also evidence that without screening one-third of all invasive breast cancers (in the age group 50 to 69 years) would not have been detected in the patient’s lifetime (Zahl et al, 2004).
natural history is still poorly understood with many never becoming invasive cancer, yet 30% of DCIS is treated with mastectomy. The charge of overdiagnosis of DCIS is selfevident. However there is also evidence that without screening one-third of all invasive breast cancers (in the age group 50 to 69 years) would not have been detected in the patient’s lifetime (Zahl et al, 2004).
Women who are overdiagnosed will have cancer treatment, which might include surgery, chemotherapy, radiotherapy and anti-oestrogen therapy. All these treatments incur costs, risks and potential harms. For example radiotherapy increases the risk of death from cardiovascular disease (CVD). Professor Michael Baum, a celebrated British surgeon, withdrew from routine screening in 1997 when the overdiagnosis issue became apparent. He has suggested that radiotherapy increases coronary heart disease risk by 30% (after 10 years). More recently Darby et al have suggested that the ‘increase [in CVD risk] is proportional to the mean dose to the heart, begins within a few years after exposure, and continues for at least 20 years.’ (Darby et al, 2013).
False positives
Across Europe the risk of a false positive for a woman undergoing biennial screening from age 50 to 69 is approximately 20%. A 2012 meta-analysis found that in the UK 2.3% of women with a false positive result had undergone a lumpectomy (Independent UK Panel on Breast Cancer Screening, 2012). These numbers are higher in the US with up to 50% experiencing a false positive at some point. After six months only 64% were given the all clear and it is only after two years that all women who had been given a false positive had been cleared (Loberg et al 2015).
Scares from false positive results can damage wellbeing for years and can also change healthcare-seeking behaviour; many people will use healthcare services more, though some will lose trust in the healthcare system (Loberg et al 2015).
False negative tests and interval cancers
An interval cancer is one detected between screening rounds. It could have been present but undetected at the last screening or it could be new and rapidly growing. As many as a third of breast cancers found at screening are in this category (Løberg et al 2015). More sensitive techniques such as digital mammography, though they would reduce false negatives, would in all probability increase the rate of false positives and overdiagnosis.
Why these differences in expert opinion?
Besides all the difficulties in interpreting screening data, I believe a major part of the answer to this question lies in publication bias. A 2007 review of the literature declared that ‘scientific articles tend to emphasise the major benefits of mammography screening over its major harms. This imbalance is related to the authors’ affiliation’ – the institutions they work for (Karsten Juhl Jørgensen et al, 2007). Others state: ‘Articles in specialty journals were more likely to explicitly reject results from the Cochrane reviews, and less likely to accept the results and methods, than articles in general medical journals. Several specialty journals are published by interest groups and some authors have vested interests in mammography screening’ (Kristine Rasmussen et al, 2013). In general, trials with negative results are twice as likely to remain unreported as those with positive results. This makes navigating the so-called ‘evidence’ extremely difficult, and can make a mockery of ‘evidence based medicine’. To find out more about this please do look at www.alltrials.net, which is calling for all trials, past and present, to be reported.
Making an informed choice
A 2003 survey of more than 4,000 women across four countries, including the UK, found that most women believed screening at least halved breast cancer mortality and that 10 years of screening would prevent at least 10 breast cancer deaths per 1,000 women (Domenighetti , 2003). Although screening information for women has improved it still overestimates benefits and underesti[1]mates the harms.
It is important that women have access to unbiased information to enable them to make an informed choice. Yet even when women are best-informed about over[1]diagnosis it does not always decrease their willingness to take part in breast screening (Waller et al, 2013). Public awareness of breast cancer and the fact that it is so common makes women fearful. And this high perception of risk must influence the decision that so many women make to continue screening despite being aware of these issues. There is some evidence to support this. One study looked at young women’s intention to screen in two scenarios: one a cervical cancer screening programme and the other a hypothetical non-cancer screening programme, with or without information on overdiagnosis. When over[1]diagnosis information was presented in the non-cancerscenario their perception of the risk of disease reduced. But in the cancer scenario information on overdiagnosis made no difference to the way they judged their risk of disease. In other words, negative emotion significantly predicted intention in the cancer group but not in the non-cancer group (Phillips et al, 2014).
Alternatives to mammography mass screening
Breast self-examination
About 80% of breast cancers not discovered by mammography are discovered by women themselves, but this is most often as part of daily living, showering, getting dressed, etc, not as part of a systematic, regular breast self-examination (BSE). In one study, only 7.6% of breast cancer patients who had practiced BSE on a regular basis actually found their breast cancers while performing BSE. Thus, it is unclear whether BSE helps women in discovering breast cancer. Some people feel that the deliberate searching makes women overly anxious about breast cancer and unnecessarily fearful about every lump that they find’
(National Cancer Coalition, 2011).
Clinical breast examination
A physical examination by an experienced professional can be a very effective tool in picking up significant breast cancers. A Canadian study found that in women aged 50 to 59, the addition of annual mammography screening to physical examination had no impact on breast cancer mortality (Miller et al, 2000).
Digital mammography
Digital mammography, which uses a lower dose of radiation, is increasingly used over film mammography. It also allows images to be enhanced and manipulated, so potentially picking up subtler changes. Nonetheless it still involves compressing the breast between two screens.
Ultrasound
Ultrasound is usually used alongside mammography in breast clinics. It is safe and user-friendly and can detect cancer at comparable rates to mammography for tumours larger than 1cm. It is, however, operator dependent – some sonographers are more skilled than others – which is a definite drawback in screening programmes.
Thermography
Because thermal imaging uses a special camera to measure the temperature at the surface of the breast, it is completely safe and non-invasive. Early functional changes such as increased blood flow and inflammation may be present several years before changes appear on a mammogram. Thermography is said to be 90% sensitive for detecting a cancer. It can identify changes even in women with dense breast tissue, though may be less reliable at picking up deeper cancers. A high false positive rate and overdiagnosis could be downsides and, though offered privately in the UK, it is generally not considered a reliable screening tool.
Targeted screening
Another approach to consider is a return to screening only those at higher risk of breast cancer, eg those with a family history and other risk factors such as obesity. This would save money and reduce overdiagnosis and false positive rates.
A different approach – healthier living
Every human being is the author of his own health or disease’.
Buddha
I believe we need to rethink prevention and management of early signs of disease. For example some scientists and practitioners of functional and lifestyle medicine have become interested in the correctable metabolic processes that underlie many chronic diseases from cardiovascular disease to cancer. Insulin resistance (IR – the hormone insulin becoming less effective) and hyperinsulinaemia (unusually high levels of circulating insulin) constitute one important root cause. The level of inflammation in the body, the health of the immune system and the diversity of the microbiome (eg the gut bacteria) are also extremely important and intimately linked.
The mainstream medical community recognises that obesity is associated with a higher risk of breast cancer and that weight loss can reduce that risk. There is obviously a large overlap between obesity and hyper[1]insulinaemia and IR, but as some slim people have similar interrelated metabolic problems, it may be that it is an underlying metabolic factor, rather than obesity itself that raises the risk. For instance we know that higher insulin levels are associated with a worse prognosis in early breast cancer and probably influence the prognosis of metastatic breast cancer (Gennari et al, 2014).
Hyperinsulinaemia and IR are not usually tested for directly, but it is related to the metabolic syndrome, which is estimated to be present in up to 25% of the UK adult population. Diagnostic criteria for the metabolic syndrome include three or more of the following: increased waist circumference; raised blood pressure; raised blood glucose and triglyceride levels and low HDL (good) cholesterol.
The charity Prevent Breast Cancer funds research into diet and lifestyle. Its most recent approach is to use two days of a low carb, low calorie diet and five days of a healthy Mediterranean diet. Their trials have found their two-day diet ‘is better than daily diets for weight loss and for lowering levels of the hormone insulin’ (Prevent Breast Cancer, 2017).
There are many versions of this sort of diet, based on real foods, high in a variety of vegetables, low in carbohy[1]drates especially wheat and sugar, high in healthy fats but avoiding processed seed oils which are pro-inflammatory. http://dietdoctor.com is one resource that I use with my patients. Some versions involve some degree of fasting, whether going several days without food or merely greatly reducing calorie intake for a couple of days a week or only eating within a six- to eight-hour window each day. All of these can be effective in normalising metabolism.
Stress reduction and exercise are also incredibly important, and, along with dietary changes, can help reduce hyperinsulinaemia and IR, as well as helping to reduce inflammation in the body, improve the health of the immune system and the microbiome.
Women need to feel empowered to take control of their own health. This starts by being given information and by having meaningful choice. I believe picking up signs of disease early can be helpful if the investigation itself is not harmful and the treatment options are going to improve health and empower the patient. A cancer ‘diagnosis’ or scare could be an opportunity for change to a healthier lifestyle. However, for this to become an affordable reality for the majority we need a paradigm shift in medicine and the NHS.
References
- Andermann A, Blancquaert I, Beauchamp S, Déry V (2008) Revisiting Wilson and Jungner in the genomic age: a review of screening criteria over the past 40 years. Bulletin of the World Health Organization, 86 (4) pp 241–320. Available at: www.who.int/bulletin/volumes/86/4/07- 050112/en (accessed 3 June 2017)
- Darby S, Ewertz M, McGale P et al (2013) Risk of ischemic heart disease in women after radiotherapy for breast cancer. N Engl J Med 368, 987–99
- Domenighetti G, D’avanzo B, Egger M, Berrino F, Perneger T, Mosconi P, Zwahlen M (2003) Women’s perception of the benefits of mammography screening: population-based survey in four countries. International Journal of Epidemiology, 32(5), pp 816–821
- Gennari A, Puntonie M, Nanni O et al (2014) Impact of insulin resistance (IR) on the prognosis of metastatic breast cancer (MBC) patients treated with first-line chemotherapy (CT). J Clin Oncol 32 (15)
- Jørgensen K, Klahn A, Gøtzsche PC (2007) Are benefits and harms in mammography screening given equal attention in scientific articles? A cross-sectional study. BMC Medicine, 5 (12)
- Løberg M, Lousdal ML, Bretthauer M and Kalager M (2015) Benefits and harms of mammography screening. Breast Cancer Research 17 (63). Available at https://breast-cancer-research.biomedcentral.com/ articles/10.1186/s13058-015-0525-z (accessed 3 June 2017)
- Miller AB, To T, Baines CJ, Wall C (2000) Canadian National Breast Screening Study-2: 13-year results of a randomized trial in women aged 50–59 years. J Natl Cancer Inst 92(18), 1490–9. Available at: www.ncbi.nlm.nih.gov/pubmed/10995804 (accessed 3 June 2017)
- National Cancer Coalition (2011) Breast self-exam: position statement. Available at: www.breastcancerdeadline2020.org/breast-cancer[1]information/breast-cancer-information-and-positions/bse-position.pdf (accessed 3 June 2017)
- NHS (2015) NHA breast screening; helping you decide. Available at: www.uhs.nhs.uk/Media/SUHTInternet/Services/BreastImagingUnit/NHS -Breast-Screening–helping-you-decide.pdf (accessed 3 June 2017)
- Nordic Cochrane Centre (2012) Screening for breast cancer with mammography. Available at: http://nordic.cochrane.org/screening[1]breast-cancer-mammography (accessed 3 June 2017
- Phillips K, Hersch J, Turner R, Jansen J, McCerrery K (2014) Exploring the ‘cancer effect’: on views about overdiagnosis and overtreatment in cervical screening among young women. Poster presentation at the 2014 Preventing Overdiagnosis conference, Oxford. Available at: www.preventingoverdiagnosis.net/2014presentations/Board%2014_Mc Caffery%20Kirsten.pdf (accessed 3 June 2017)
- Prevent Breast Cancer (2017). Diet and lifestyle. Available at: https://preventbreastcancer.org.uk/breast-cancer-research/research[1]projects/diet-and-lifestyle (accessed 3 June 201
- Rasmussen K, Jorgensen KJ, Gotzsche PC (2013) Citations of scientific results and conflicts of interest: the case of mammography screening. Evid Based Med 18(3), 83–9
- The Independent UK Panel on Breast Cancer Screening (2012) The benefits and harms of breast cancer screening: an independent review. London: Screening Cancer Research UK and DoH. Available at: www.cancerresearchuk.org/sites/default/files/ibsr-fullreport.pdf (accessed 3 June 2017)
- Waller J, Douglas E, Whitaker KL, Wardle J (2013) Women’s responses to information about overdiagnosis in the UK breast cancer screening programme: a qualitative study. BMJ Open. Available at: http://bmjopen.bmj.com/content/3/4/e002703 (accessed 3 June 2017)
- Zahl PH, Strand BH, Maehlen J (2004) Incidence of breast cancer in Norway and Sweden during introduction of nationwide screening: prospective cohort study. BMJ, 328, 921–924






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}