

Activating hope in times of unravelling
Chris Johnstone, Resilience specialist, CollegeOfWellbeing.com
Published in JHH16.2 – Faith, hope and love in healthcare
I trained as a GP, then for many years worked as part of a specialist mental health team treating people with alcohol dependence.These days I teach online courses about wellbeing, active hope and resilience. My books include Active Hope (co-authored with Joanna Macy and translated into several languages), and Seven Ways to Build Resilience.
DP – Hope is a central theme for this edition and also of Active Hope, the book you co-authored with Joanna Macy. How do you see hope and why is it important?
Something I’m deeply interested in is what help us more fully engage in life, with its ups and downs, and challenges, in ways that contribute to wellbeing not just of ourselves, but also of the world around us. Hope is part of the story here. But it is not straightfoward – because while some aspects of hope can be enlivening and draw us more into life, the opposite is possible too. For example, if we think we need to have hope before we can follow a purpose, what happens when we lose hope? Do we give up on our purpose too? At a time when so many people struggle to feel hopeful about the future, whether their own, or that of the world around them, we need a different approach.
DP – so what is active hope and how is it helpful?
The word hope has different meanings. In the question ‘are you hopeful?’, you’re asking someone about their assessment of how likely something is. Is it going to work out? or not? Do you have your hopes up or not? Compare that with the question ‘what do you hope for?’ Here you’re inviting them to tell you about their desires and preferences. Active hope is more to do with this second meaning and it involves three key steps. First you start from where you are, being fully present to the reality of your starting point. Then, you identify what you hope for from there – what’s the direction you’d like things to move in? And third, you take steps that way, you’re active in the process of making your hoped-for future more likely.
DP – how has this perspective been useful in your work as a medical doctor?
For much of my medical career, I worked with people with severe alcohol dependence. When someone stops drinking, and begins recovery, there’s all kinds of hopes generated about how things might go – both for the client and also for any helping professionals involved. When a relapse happens, those hopes get dashed and that can be hugely painful. I often saw clients who, after repeated relapses, felt such a sense of hopelessness that they’d say, ‘What’s the point? I keep failing. It’s not going to work, I can’t do it’. One told me he’d given up giving up, because it was too painful to keep on trying when each time he fell flat on his face.
Yet working in groups, other clients would say things like, ‘I was like that a few months ago, and then something changed. I hated being so disappointed with myself, I hated how I felt, being so out of control, I reached a point where I’d do anything to get well. I learned I just had to take it a bit at a time, sometimes even five minutes or an hour at a time. Doing that, I got through a whole day, then another one. Building on that, things gradually changed.’
There’s something here about having a light at the end of the tunnel, then losing that light, then finding a way. How do we keep going even where we’re not sure where the light is? Active hope starts from the recognition that whatever you face, there’s different ways it can go. Even if there’s no light at the end of the tunnel, there will be different versions of being in a lightless tunnel, some of these better than others. To represent this, I use an image I call the spider diagram. If the body of the spider represents the present moment, then each leg is a different way the future can go. What’s the best way things can go from here? What’s the worst? And what’s most likely? These questions point us to different legs. Active hope is about taking steps to make the best more likely, and the worst less so. From whatever starting point you have, you begin from there, and identify your preferred legs of the spider – your hopes about how things will go. Then you head that way.
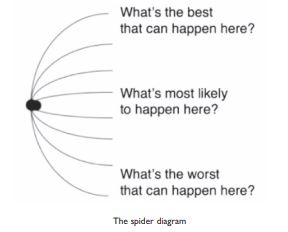 For someone giving up drinking, their hopes about where recovery might lead are like the lights at the end of the tunnel. But when things are so bleak that no lights are visible, they can still recognise some legs of the spider as more hoped for than others. When really struggling, just getting through five minutes without drinking is a better leg of the spider. Active hope is about what you do to make that more likely. It might be phoning for support. It might be pouring a bottle you have down the sink, rather than drink it, because you’re not sure you’d be able to resist it if you still had it around. What we’re looking at here is hope as a direction rather than a place. The light at the end of a tunnel is a place, and hopefulness is about how much we believe we might get there. I was working with people who didn’t feel hopeful at all, where the idea of being well and happy in a stable recovery seemed impossibly far away. If they thought about hope in terms of ‘will I get there?’ it was depressing and left them wondering what the point was. But if they thought about hope as a direction they could move in from any starting point, and active hope as the process of moving that way, it became something they could succeed in every day. It became doable.
For someone giving up drinking, their hopes about where recovery might lead are like the lights at the end of the tunnel. But when things are so bleak that no lights are visible, they can still recognise some legs of the spider as more hoped for than others. When really struggling, just getting through five minutes without drinking is a better leg of the spider. Active hope is about what you do to make that more likely. It might be phoning for support. It might be pouring a bottle you have down the sink, rather than drink it, because you’re not sure you’d be able to resist it if you still had it around. What we’re looking at here is hope as a direction rather than a place. The light at the end of a tunnel is a place, and hopefulness is about how much we believe we might get there. I was working with people who didn’t feel hopeful at all, where the idea of being well and happy in a stable recovery seemed impossibly far away. If they thought about hope in terms of ‘will I get there?’ it was depressing and left them wondering what the point was. But if they thought about hope as a direction they could move in from any starting point, and active hope as the process of moving that way, it became something they could succeed in every day. It became doable.
DP – how does this active hope process apply in other areas of medicine?.
With something like severe asthma, you can feel quite out of control. You can hope like anything that you won’t get a bad attack. But there’s a difference between passive hope and active hope. Passive hope is hoping for the best, but not playing a role to help that happen. Active hope involves looking at what you can do to make your hopes more likely. Even when a condition feels out of our control, there will still be ways you can influence what happens. The key thing is to identify choice-points where going one way rather than another has an impact, even if just a small one, on what happens. With asthma, it might be learning more about triggers and preventative measures. Research shows, for example, that practising self-hypnosis can reduce the severity and frequency of attacks.
A big challenge with self-help strategies is that you can take the steps, but not always see an immediate benefit. You can do self-hypnosis and aim to avoid triggers, yet still have an asthma attack. It is easy to get disillusioned if our actions don’t lead to the results we hope for.
DP – How can you trust that what you do is worth the effort when it doesn’t seem to work as you’d hoped?
I think what’s needed here is a different way of thinking about cause and effect. A piece of advice often found in self-help books is ‘focus on what’s in your control’. But I find influence a more helpful concept than control. The challenge is that recovery in long-term health conditions – whether asthma, addiction, depression or heart disease – is a complex process involving many different factors. It isn’t as simple as ‘A causes B’ in that if I do A, that will control my symptoms and cause my recovery in a direct, easily-seen way. Often the impact of a self-help practice is subtle; each step you take adds to a context that can help shift a larger balance. For example, in the diagram below, which square causes the circle?
It isn’t a single square that does it, but rather the circle emerges out of a number of squares acting together as a whole. Even three or four squares aren’t enough – you need to reach a critical threshold or tipping point where enough of them acting together creates the shift from some squares to a circle of squares. What we’re looking at here is systems thinking, where larger patterns or processes emerge from smaller elements acting together as a whole. This leads to a different way of thinking about cause and effect. Rather than looking for the cause, you look at contributing causes that act together, leading to the emergence of a more visible effect.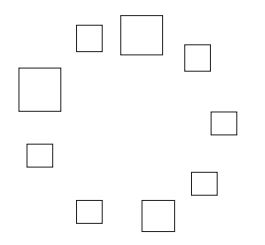
Each square, when arranged a particular way, adds to a context that makes the circle more likely. This way of understanding causation is in the form of ‘A (an action) adds to a context that makes B (a consequence) more likely’. The regular practice of self-hypnosis adds to a context that makes longer periods without asthma attacks more likely. Going to a recovery support group isn’t enough by itself to stop someone drinking, but it can add to a context that makes recovery more likely. Like with the squares, we often need several things acting together to tip the balance towards recovery
DP – Taking a jump from the personal to a team or organisational level, how might this way of thinking about cause and effect help health professionals who are experiencing despair about their working conditions?
Thirty years ago, I was in despair as a junior doctor working more than 110 hours some weeks – in a busy job where I was up for much of the night after working the previous day, and then expected to work during the next day too. It was ridiculous. When I asked my colleagues what we could do to improve conditions, they replied ‘we don’t have the power here, there’s nothing we can do’. I know that’s how many people working in the public sector feel right now, with years of cutbacks stretching services too far.
I’d been interested for many years in the process of how change happens, not just at a personal level, but also in cultures, organisations and society. The perspective of ‘A adds to a context that makes B more likely’ got me interested in how I could play my part in supporting a context that made changes we wanted more likely. So back then I joined a small group of doctors campaigning on this issue. We slept overnight on the pavement outside The Royal London Hospital, attracting press coverage that raised the issue in the political agenda. Eventually I took my health authority to court, challenging the legal basis of my contract. After six years going through the courts, I eventually won the case. It had a huge impact.
When I started my court case, my actions were seen as courageous but foolhardy. I was dismissed as an unrealistic dreamer, as my case was widely seen as unwinnable. But my experience taught me to have a more open mind about what is realistic or possible. The view that something can’t happen is an assessment based on what we know at the time. It isn’t necessarily a statement of fact.
In systems terms, it’s interesting to consider what features of a context we can add to. Great questions here are ‘what happens through us’ and ‘what are we part of?’. The collective response happening through many of my colleagues about the doctors’ hours issue was one of acquiescence. That added to a context that made it more likely the problem would continue. What kept me going was a determination to express a different response. I wanted to use my influence the best way I could. Even though I wasn’t sure that my actions, by themselves, would add up to much, when I thought ‘what are my actions part of?’ I felt part of a long tradition of people who’ve stood up for change, who’ve initially been dismissed, but who hung on in there in a way that helped shifts happen. I felt part of a powerful story that involved many other people, not just me. Like the squares being part of the circle, I was showing up in an attempt to help a different pattern emerge. So the question I explore in addressing working conditions or any other issue, is ‘what would a story of change look like here, and how can I play a part in that?
DP – How can this perspective on hope be useful when facing issues like climate change?
The starting point for me is the spider diagram. Whatever we face, there are different ways it can go. What’s the best that can happen? What’s the worst? And what’s most likely? Then how can we make the best more likely, and the worst less so. The worst that can happen is really awful. What’s most likely, if we carry on the way we’re going, is very scary too. Yet even from a lower leg of the spider, it can still go different ways. In my resilience training work, I draw this as a double spider – where we look at the range of possibilities when things have already taken a turn for the worse. My work is about looking at what supports us to rise to the occasion when facing difficult times, and how we can play our part in making a better version of what comes next more likely.
When we’re in a dip, whether in our personal lives, our workplace situation, or collectively with the world, we can’t know whether our efforts will bring about a turning towards the better future we hope for. Joanna Macy, my co-author with Active Hope, uses the phrase ‘radical uncertainty’ to describe a state of openness to possibility, where it’s our not knowing whether things will get better or worse that provokes us to show up and use our choices to steer the flow of how things develop. Will we get there? Who knows? But if we see hope as a direction that really matters to us, that can activate us to take steps that way.






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}