

Wise doctors: What can they teach us about flourishing?
Sabena Jameel GP and Medical Professionalism Lead, University of Birmingham Medical School
Published in JHH18.1 – Flourishing in Medical Education
For me, the ultimate continuing personal and professional development is to seek what it is to be wise. Not just clever, not just efficient, but wise. This turns traditional medical education on its head. Embedded in the concept of wisdom is a moral orientation towards good… a flourishing of self and others. I believe this lofty nirvana is achievable. Careful career crafting has enabled me to achieve an exciting position of being both a practitioner (GP) and a clinical academic responsible for professionalism education in a large UK medical school. A seven-year PhD quest to capture what enacted wisdom looks like in general practitioners has been a most fulfilling part of that journey. That is what I whole-heartedly want to share with you.
In Nichomachean Ethics Aristotle asserts that there are five excellences of knowledge, sometimes called intellectual virtues (Aristotle, 2004). Episteme is scientific knowledge, techne is technical expertise, sophia is philosophical wisdom and nous is intellectual insight. The fifth is less well understood, although it has been suggested that this virtue is of particular use to those in medical practice (Pelligrino &Thomasma, 1993). This virtue is phronesis (practical wisdom). Over the last three decades theoretical musings suggest phronesis is synonymous with professionalism (Kinghorn, 2010; Hilton & Slotnick, 2005), emphasising a moral orientation towards good rather than reductive standards set by regulators with punitive consequences for non-adherence. On this basis alone it would be worthy of study, but what is even more appealing is the Aristotelian hypothesis suggests that developing phronesis is a step towards eudaimonia (flourishing of self and others). In this climate of burnout and demoralisation in clinical practice we owe it to ourselves to explore phronesis in medicine.
Medicine is a natural science, rich in bioscientific experimentation leading to rules and laws that help us understand the world. It is also a human science full of constructed understandings of how and why things happen generating emotion and values. This has been captured nicely in the aphorism from Kaldjian (Kaldjian, 2019) not exclusively for the older age group… and not all old people are wise. High levels of self-awareness and constructive growth-orientated reflection are key, as opposed to ruminative, pessimistic reflection. This resonates with wisdom research by Meeks & Jeste (2009).
Medicine is the most human of sciences and the most scientific of the humanities.
In order to perform well in medicine, the deductive aspects need to be paired with the interpretive aspects. Phronesis offers an appreciation of both aspects. The rational orientation of bioscience synthesised with the skill of contextual clinical judgement (Gatens-Robinson, 1986). Phronesis is rooted in virtue ethics as opposed to the rule-based ethics that dominate healthcare. Phronesis is a meta-virtue that adjudicates when values conflict, it is inherently practical. To date very little empirical work has been published about phronesis in medical practice (Kotzee et al, 2016). This was the starting point for my PhD research on enacted phronesis in general practitioners.
The research aspired to capture the lives, thinking habits and actions of wisdom exemplars. Too much of professionalism research focuses on bad behaviour and poor professionalism. When used in medical education, I hoped that the narratives from empirically derived wisdom exemplars would help clinicians understand something of themselves when reflecting on the narratives. My hope was that the exemplars could become role models, raising aspirations towards excellence. These stories are fascinating as standalone lessons, but the PhD research went on to look for common themes.
In 2016–2017 211 GP trainers completed a wisdom questionnaire at various GP training events. There was no compulsion to complete the questionnaire. The overall response rate from the training events was 57%. The wisdom questionnaire was a measure of wisdom that best approximated to phronesis (Ardelt, 2003) as there is, to date, no measurement tool to measure phronesis (Kristjánsson, 2020).
Ardelt (2003) built a scale with the cognitive, reflective and compassionate indicators that measures the latent variable of wisdom in large standardised surveyed populations. I selected the highest scoring respondents with a strong criterion for wisdom in each of the three domains (approx. 10%) to participate in the second part of the study, the biographic narrative interviews. The interview technique and panel narrative synthesis followed the biographic narrative method (BNIM) described by Wengraf (Wengraf, 2001). The analysis focused on the lived life and the told story of the exemplar. Each interview resulted in a narrative output statement. This article presents four of these eighteen biographies.
Samphire
Samphire grew up in a tense household describing parental aggression and neglect. Success at comprehensive school meant she escaped home, enjoying medical school and university life. Her natural curiosity for people led her to general practice. Continuity of care and the prospect of a better work–life balance were key factors. The entirety of Samphire’s working life has been marred by episodes of sexism, initially while looking for GP partnerships in the 1990s, right up to the bullish management boards she sits on now. Her husband too was met with disdain when he chose to be a house husband. Samphire spent a sabbatical with her family abroad; this was an interesting adventure. Samphire values her primary care team; they have been through difficult times together. Samphire learnt to trust herself, gaining confidence in her own abilities. She is acutely aware and conscious about giving patients the ability to speak and be heard. This is a trait she transfers to her family too. Samphire feels that a person’s behaviour can affect the feelings of others. She knows how she would like to impact others. She enjoys delivering practical teaching to trainees, focusing on process, and planning rather than the fixation on diagnoses. Her role as a carer for her mum (RIP) and her children has enhanced her ability to be a better doctor.
Lulu
Lulu’s journey to phronesis has involved aligning her acute awareness of self and understanding herself with the boundaries and infrastructures that needed to be put in place to bring her to a point of joy and happiness in her work as a GP.
This journey has involved quite intense and painful experiences as a carer for her mother and her own child. She is also a patient with two life-changing diagnoses and has experiences being an unsupported junior doctor who required time out for perceived burnout. She navigates through these events with insight, knowing what she did not want to be like and working towards being the doctor she wanted to always become. Parents, spouse, pets, and colleagues now strengthen her, like the armour she needed to enhance her own abilities. Her experiences had taught her a lot, though she would not re-live them. Lulu has demonstrated humble resilience and continues to practise medicine in a humane way, knowing how much it has taken for patients to open up to her. That privilege is something she values and drives her to do onto others as she would want for herself – kindness, compassion, and connection.
Billy
Billy relates a life that started with an apparent failure, being labelled ‘thick, hyperactive loner’ in childhood. Key figures believed in him and empowered him, putting him in a more favourable environment for growth and development. He thrived, despite some challenges in his childhood and teenage years. He was able to filter the negative perceptions and work with the positive comments and his own reflective thought processes and cognitive reasoning about life and purpose. He finds a strong sense of achievement in making connections and understanding others. He found the caring role rewarding even from a young age. He loves breadth of intellectual stimulation. He remains indebted to his parents and reflects on this through his own journey of being a parent.
Dolan
Dolan’s narrative illustrates a quest to transcend and under[1]stand the challenges he has faced through life. He adopts an external observer perspective, using philosophical concepts to help him reconcile challenges to his perception of what justice and fairness should be. He wants to do himself justice in a system that is not just. This understanding extends to patients too. His perception of injustice is from a long series of events that started in childhood. Dolan is deeply reflective and ‘navigates’ his way through with high levels of intelligence and as a tactician. He seeks meaning and purpose.
What do you feel as you read these statements? Can you relate to any of the narratives? What are your take home messages? What is striking is how each exemplar has faced challenge and difficulty, but they exhibit thoughtful resilience and an ability to learn and grow. Their reflection is not ruminative but proactive in improvement. They strive to be the best version of themselves, not showing much interest in competition with others. Contrast this to the award/prize/promotion rat-race culture that currently defines success in a medical career. Their motivation is internal, not external. They have learnt to ignore the naysayers and critics; this is particularly noticeable in the narratives of Billy and Samphire.
The exemplars have a strong sense of autonomy in directing who they want to be and how they would like that to play out. They are self-assured but humble, strong yet vulnerable. Wisdom does not mean perfection; it means work-in-progress with a humane love for others and an orientation towards good. The exemplars often disclose a personal close relationship and/or personal illness which seems to have shaped their own capacity for compassion. In the case of Samphire and Dolan it was as a result of experiencing harsh treatment themselves that they set out to consciously provide something better than they had endured.
For Lulu it was her own medical diagnoses. Lulu learnt to use healthy boundaries and loved ones to strengthen her own compassion. Many exemplars tacitly follow the golden rule, ‘do unto others as you would have them do unto you’ – this guides their behaviour with patients. What is fascinating about the age range of the wisdom exemplars are that it included young people (late 20s), who were newly qualified GPs. Lulu was one of those exemplars. Wisdom has been shown to increase with age, but it is not exclusively for the older age group… and not all old people are wise. High levels of self-awareness and constructive growth-orientated reflection are key, as opposed to ruminative, pessimistic reflection. This resonates with wisdom research by Meeks & Jeste (2009).
Not immediately evident from the four narratives in this article, but as themes from all the exemplars narratives, is the ability to deal with uncertainty. This seems to be a defining feature of the wise. This research also involved interviewing a couple of low scoring GPs. Their indecision and torment in dealing with uncertainty was evident. Doubts and indecision came through repeatedly. One low scoring exemplar attributed much of his life to luck, using the word 28 times during the interview and suggesting an external locus of control. The high scoring exemplars gave the impression of personal agency and self-determination, often surprising themselves with their capabilities when they were put in situations of high challenge. Many of the wisdom exemplars described themselves as average at medical school. It begs the question as to whether we are measuring the right thing at medical school. Should we be looking at wisdom rather than knowledge? Analysing both low scoring and high scoring GPs brought the quote by Chia & Holt to life.
We develop the idea of wisdom as a form of learned ignorance – a cultivated humility, meekness of demeanour, and openness of mind that is distinct and different from the aggressive and relentless pursuit, acquisition, and exploitation of knowledge. Rather than associate wisdom with learning, we argue that it is ironically unlearning that is the path toward genuine wisdom and insight. The inability to attain wisdom arises, paradoxically, from a contemporary obsession with knowledge and information. Wisdom is not about having more information or constructing irrefutable propositions. True wisdom exceeds these quantifiable elements. It takes its cue from vagueness and ambiguity.’ (Chia & Holt, 2007, p505).
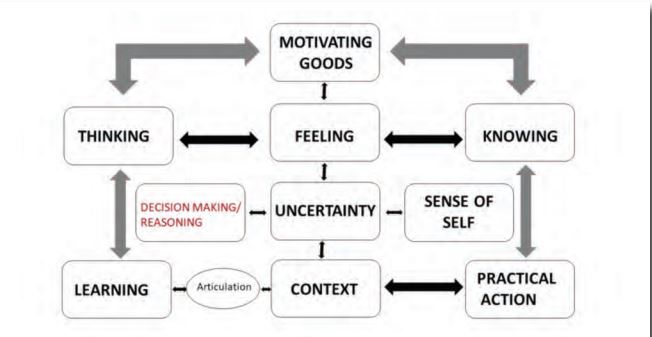
Corpus linguistic software was used on all 18 transcripts. This highlighted the main discussion themes (filler words excluded). It enabled a conceptual framework for wisdom in action to be developed. The inter relationships and feedback loops are illustrated in the diagram below. It shows how thinking, feeling, and knowing are influenced by motivations. Thinking, feeling, and knowing also determine the perception of our self, which in turn affects our reasoning/decision making ability and our ability to deal with uncertainty. Our thinking and subsequent reflection affects our ability to learn. All this happens in context. This is a defining feature of phronesis. All these features together feed into practical action. Practical action (praxis) is the end point of how practical wisdom manifests.
Wisdom does not mean perfection; it means work-in progress with a humane love for others and an orientation towards good
Phronesis is about doing the right thing, at the right time, for the right reason (Schwartz & Sharpe, 2010). It is inherently contextual, and this is in contrast to the generalisable reductive rules, guidelines, and protocol[1]based approach to clinical medicine. This research was most fulfilling. The stories from the wisdom exemplars are memorable and engaging. It is about real clinicians who are flourishing. The exemplars were generous with their time and candid in their narrations. The icing on the cake was when the quantitative part of the study asked a specific question on satisfaction and contentment. There was a clear correlation between a high wisdom score and a sense of wellbeing. This supports Aristotle’s theory that developing phronesis is a route to eudaimonia (flourishing). I hope that further work will allow an even more nuanced appreciation of phronesis and how to achieve it.
Too much of professionalism research focuses on bad behaviour and poor professionalism
When I have used these biographic narratives in teaching sessions with GP trainers and trainees, their responses have included how, despite challenge, the exemplars remain positive. Many could relate to the stories of the exemplars and as a result felt inspired.
Sabena’s teaching last week was really thought provoking, she is a charismatic speaker whose passion for the topic really engaged the audience. The other trainees also said they were impressed and were interested in the subject of phronesis which was explained very well. The case studies of each exemplar were insightful showing the common themes in their lives that have led to wisdom. It is interesting to note that wisdom seems to be correlated with job satisfaction; is there causality? Some questions raised included “If phronesis could be taught would it make us better GPs? Does choosing a career in GP preselect predominantly wise doctors?” I think the talk naturally inspired us to reflect on our own practice and lives in general.
It was an incredible session on phronesis. Definitely an amazing take on being a GP. I think every cohort at VTS training should hear this and be part of it and be inspired. Thanks for organising it. One of the best VTS session.
Their feedback speaks volumes. The time is right for understanding and teaching wisdom. We need to learn how to flourish, now more than ever.
REFERENCES
- Ardelt M (2003) Empirical assessment of a three-dimensional wisdom scale. Research on Aging, 25(3) 275–324.
- Aristotle (2004) The Nichomachean ethics (translated). Penguin Books.
- Chia R & Holt R (2007) Wisdom as learned ignorance: integrating east-west perspectives. In Kessler EHE & Bailey JR (eds) Handbook of organizational and managerial wisdom. Sage.
- Gatens-Robinson E (1986) Clinical judgment and the rationality of the human sciences. The Journal of Medicine and Philosophy: A Forum for Bioethics and Philosophy of Medicine, 11(2) 167–178.
- Hilton S & Slotnick H (2005) Proto-professionalism: how professionalisation occurs across the continuum of medical education. Med Educ, 39(1) 58–65.
- Kaldjian L (2019) Wisdom in medical decision-making. In Glück J & Sternberg RJ (eds) The Cambridge handbook of wisdom. Cambridge University Press.
- Kinghorn WA (2010) Medical education as moral formation. An Aristotelian account of medical professionalism. Perspectives in Biology and Medicine, 53(1), 87–105.
- Kotzee B, Paton A & Conroy M (2016) Towards an empirically informed account of phronesis in medicine. Perspectives in Biology and Medicine, 59(3) 337–350.
- Kristjánsson K (2020) An introduction to the special issue on wisdom and moral education. Journal of Moral Education, 49(1) 1–8.
- Meeks T W & Jeste DV (2009) Neurobiology of wisdom?: A literature overview. Archives of general psychiatry, 66(4) 355–365.
- Pelligrino E & Thomasma D (1993) The virtues in medical practice. Oxford University Press.
- Schwartz B & Sharpe K (2010) Practical wisdom – The right way to do the right thing. Riverhead Books.
- Wengraf T (2001) Qualitative research interviewing (1st edn). Sage.






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}