
Until the last breath
Shakira Irfan, Third year medical student, St Georges University of London
Published in JHH18.1 – Flourishing in Medical Education
What does it mean to be human?’ is a question I find myself asking every day. Reflective practice through my journey as a medical student forces me to break down the walls that allow us to sit comfortably within structured consultation and a checklist of questions. This piece is inspired by the very essence of what makes us unique, especially at our most vulnerable. I wanted to explore a patient perspective that demands the most humane aspect of medicine: listening.
The journey to medical school is often met with the question, ‘Why do you want to study medicine?’. It forces prospective students to uncover their personal and genuine interest to work in healthcare and confront the experiences that make us both vulnerable and determined. Beyond the knowledge of science, human anatomy and medicine that is taught in the years that follow, nothing can truly prepare a student for the unfiltered sense of humanity that a career in healthcare entails. From beginning a journey of self-discovery to appreciate that doctors are also human, to unpacking the complexity of human behaviour and emotion in patients, the answer to the question ‘why medicine?’ is ever blooming.
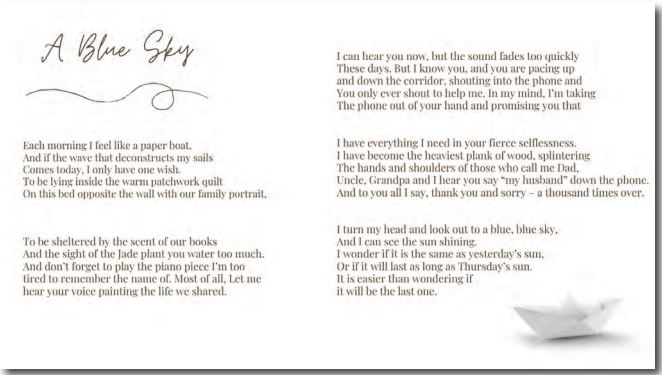
My poem A Blue Sky explores the unfettered nature of the human condition through the perspective of an elderly male approaching the end of his life. Inspired by Dr Graham Easton’s The Appointment, which provides an insight into a doctor’s mind through 18 GP consultations, this poem delves into a perspective that aims to break down the rigid, tick-box way of interacting with a patient that students can fall into, by observing each patient as their own person with individual needs.
Not having grown up with either of my grandparents, end of life care is an unfamiliar aspect of medicine. A patient can be considered approaching the end of life if they are likely to die within the next 12 months. The decision to focus on this aspect of healthcare stemmed from considering the need for doctors to amplify patient voices during a notably vulnerable time, while redefining what end of life care means on a personal level (General Medical Council, 2010).
The comparison of the patient to a paper boat is an extended metaphor for the fragility of life. It encompasses the inevitable unravelling of a youthful construct to high[1]light the uncertainty of death for a patient, where they are aware of an end, but may be unsure exactly when and how this may happen. This provides a huge opportunity to appreciate human fear and helplessness, a reality that is difficult to convey in mock clinical scenarios with peers of the same age. As the poem progresses, the patient high[1]lights his wishes such as wanting to pass away in the comfort of his home, where he can lie in the patchwork quilt and see his family portrait. This brings to light how every patient a student or doctor will encounter has their own story, a lifetime of moments that piece together the parts of who they are, countless journeys that influence the ways they think and feel, and personal needs that make them fiercely human.
In stanza two, the patient dives into his personal needs. Where one patient may choose to die at home, another may want to be in a care home or hospice. Where this patient wants to hear the piano, another may choose to be surrounded by the sound of the Qur’an, hymns, a playlist of meaningful songs, or have a religious figure in the room. The persona wants the familiarity of his daily life, the sights, scents and sounds that upkeep his norm, which raises a significant point about ensuring that patients are not just surviving, but are in fact living. Dame Cicely Saunders, the mother of palliative care in modern medicine, beautifully captures this in her own words: ‘You matter because you are you, and you matter to the end of your life. We will do all we can not only to help you die peacefully, but also to live until you die’ (Twycross, 2006). Patients are not just vessels to pump medication into for a chance at another day, but human beings with complex emotional, physical, mental, medical, and potentially religious needs, highlighting the need to treat the patient holistically. It encourages an important viewpoint, which is that we are not just unique in life, but we are also unique in death and patient dignity, comfort and humanity should be at the forefront of care from the cradle until the last breath.
The poem further explores the complex nature of end of life such as the emotions experienced by the patient: love, pain, guilt and hope, underlining the need for a very human approach to end of life care. The persona experiences feelings of guilt and gratitude, apologising and thanking members of his family in turn, to show how this is an emotionally complicated experience for patients and their families. It sparks interesting discussions regarding the possible Eastern-Western divide in caring for the elderly and the ways culture, traditions and expectations can influence palliative care. We can understand the limitations of a doctor and pinpoint a sensitive balance between providing medical care and providing a deeply compassionate form of holistic care that includes all aspects of the patient’s life, such as supporting their families. Medicine is nuanced and the words ‘end of life’ may almost immediately illustrate an elderly person in the minds of readers, but this is a reality for children and young people, which adds an additional layer of complexity and unique needs, to demonstrate that medicine isn’t concerned with stock-type characters, but rather starkly different people with individualised approaches to life. While tending to patients’ medical needs, it is important not to solely provide a medically designed answer to unfixable problems, a life designed to be safe but empty of anything they care about’ (Gawande 2014, p109).
Conversations with doctors in palliative medicine high[1]lighted the stereotype of this being a dark or upsetting specialty, when in daily practice it is profound and hopeful and marks the most valuable times in a patient’s life. Through the ebb and flow of difficulty and moments of light, an untainted sense of what it means to be a human being is brought to the surface. This is difficult to replicate in artificial educational settings, but important to understand even before experiencing our very own consultations. Through discussions, observation, and the power of literature, I, as a student, have enhanced my outlook and practice to value human life through a lens that appreciates the unapologetic desire to feel human in the face of difficulty and to understand that every single one of us has a story.
References
- Gawande A (2014) Being mortal: Medicine and what matters in the end. Metropolitan Books/Henry Holt and Company.
- General Medical Council (2010) Treatment and care towards the end of life: good practice in decision making. General Medical Council.
- Twycross R (2006) A tribute to dame Cicely Saunders. St Christopher’s Hospice. www.stchristophers.org.uk/about/damecicelysaunders/tributes (accessed 8 March 2021).






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}