
The living gap – bridged by life-compassion: first order principles for healing the crises of our planet, its peoples, and you
David Reilly, Director, The WEL Project
Published in JHH 19.1 – Integrative Medicine
First order principles:
350 BC Aristotle: ‘The first basis from which a thing is known.’
Cannot be deduced (reasoned, worked out) from any other proposition or assumption.
The fundamental concepts or assumptions on which a theory, system, or method is based.
Wisdom is truth independent of scale and time. If we can distil robust first order principles for healing and health, they can serve as compass headings to navigate crises and illness into recovery, wellness, and flourishing – even in uncharted challenges. Such guiding principles need to be based on their evident effectiveness. At best, their self evident truth chimes with shared instinctive values to foster collective understanding to help bring us back on course. If sound, they shed light on deeper root causes and needed actions in breakdown and crises of health across the scale of the planet, its peoples, and each of us personally.
To be useful, the principles we seek must be simple, but not simplistic clichés or slogans. They are complex simplifications of patterns. Direct observation of nature in action is central here. Yet things simple in essence can be hard in application – like caring for ourselves, or our planet.
I hope to support your own reflections and emerging insights by offering some examples from my enquiry. Before reading my ideas, perhaps take a moment to reflect: what are your core guiding principles?
Creating such principles is a tall order, and a usefully hard task. My own learning has been rooted in enquiring as deeply as I could throughout my life as a clinical doctor into the stories of what determined individual people’s shifts into decline and recovery, in the short term, and over their life course. In particular, I focused on detailed study of individual patients who had experienced periods of evident improvement and healing, without any other medical intervention. I then endeavoured to apply this learning to inform and improve my care, research, and teaching.
I learned how bringing sound principles can act as a catalyst in therapeutic process, triggering their interacting with the surrounding contexts of internal and external environments, and of human connection and so the world of inner experience and meaning. For example, with my colleague Stewart Mercer we saw how experiencing empathy is a prerequisite for successfully enabling a patient into better self-care. (Mercer et al, 2001). Such first order principles can then help us create therapeutic consultations (Reilly, 2001a) and then use the resources this releases to cut through confusion and inspire and encourage personal and collective actions.
A couple of decades into this work, I explored scaling up the learning into a group-based course built primarily on the central principles of health and healing, rather than on informational transfer (TheWEL Course). I was making progress but was then pushed out of my clinician’s comfort zone by Phil Hanlon, Professor of Public Health at the University of Glasgow. He asked if we could join forces to see if the principles derived from my one-to-one field studies could be applied in public health. In 1999, Phil joined me as I consulted with ‘Paul’ who described a transformative healing reaction triggered by his previous therapeutic consultation. Phil was taken aback by the power, depth, and speed of change that Paul described and asked me: ‘How can we take what we have just seen and scale it to the level of a nation?’ Since then, his wonderfully challenging question has spurred me on in identifying scale-independent first principles for healing and flourishing. I now offer you that same challenge.
The sister challenge is the art of then effectively sharing these principles. It requires more than words and logic, but also right-brain imagery as intuitively clear as the principles themselves. If wisdom can be faithfully double distilled down to be transmitted in just a few words, an aphorism, or an image – all to the good. Often our universally shared descriptions of nature in action are effective. A bit like Bono who described his lyrics as ‘ending up sounding like a weather report’. Such attempts at representing first order principles are scattered throughout this article. Scan for them as you read on.
Icon: A sign with some factor in common with the object it represents. (Shorter Oxford English Dictionary, Oxford University Press, 2007)
Let’s begin with an image chosen to symbolise some of the principles we will be exploring. How it does so will, I hope, become more apparent as we progress. For now, what, if anything, do you ‘read’ in this image; and what feelings or instinctive responses are activated as you look into the eyes of this child?
Now, let’s begin our journey from where we are: any other approach to travel is not recommended.
‘The pandemic soil’
The seed of ill-health germinates in the soil of context. As the Covid-19 pandemic began, it quickly became evident that almost all people admitted to an intensive care unit in New York had predisposing conditions, 94% had one, and 88% two (Richardson et al, 2020). Time has confirmed that the cardinal risk factors for severe disease and death, after age, are being overweight or diabetic (Kompaniyets et al, 2021).
For decades before Covid we have seen an ever-rising tide of pandemics of long-term and degenerative conditions (aka non-communicable diseases – NCDs) especially in ‘developed’ countries.
This second image is an icon of these global pandemics in microcosm.
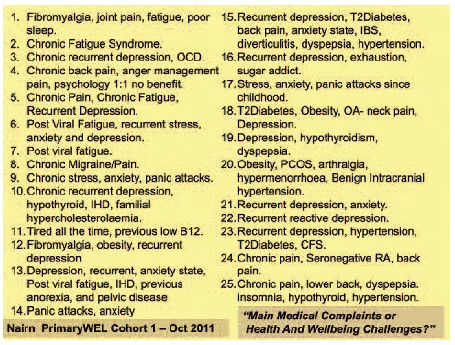 It shows the health and wellbeing challenges of 25 people who entered a programme aimed at helping them cope with their NCDs and make long-term, self-sustaining shifts in their self-care and so improve their wellness (Reilly, 2004–21). We can see here the state of the soil 10 years before the viral seed of Covid landed. Note also that if you develop one of these conditions, you’ll probably get several. We typically descend through loss of wellbeing into long-term impairments of health before next-level consequences like heart attacks, strokes, and cancers. These late-stage diseases affect more than 50% of adults, at increasingly earlier ages; some, like diabetes, are even spreading to our children. While medical advances have improved outcomes, they have not slowed this progressive and worldwide decline in health and wellbeing, nor can they alleviate all the suffering it brings. This predicament needs so much more than medical solutions.
It shows the health and wellbeing challenges of 25 people who entered a programme aimed at helping them cope with their NCDs and make long-term, self-sustaining shifts in their self-care and so improve their wellness (Reilly, 2004–21). We can see here the state of the soil 10 years before the viral seed of Covid landed. Note also that if you develop one of these conditions, you’ll probably get several. We typically descend through loss of wellbeing into long-term impairments of health before next-level consequences like heart attacks, strokes, and cancers. These late-stage diseases affect more than 50% of adults, at increasingly earlier ages; some, like diabetes, are even spreading to our children. While medical advances have improved outcomes, they have not slowed this progressive and worldwide decline in health and wellbeing, nor can they alleviate all the suffering it brings. This predicament needs so much more than medical solutions.
Suffering is not the enemy, it is the call for change
Suffering can be a warning signal guiding us to needed change. Symptom control may be necessary, but don’t use it to just cut the wires to these warning lights. Suffering can be used to wake us up to being on the wrong course, and so question our compass settings. Shall we take notice and alter course, or just medicate or addictively numb our symptoms and forge on? Suffering can lead us to ask if our way of living is working for us? Will our personal and communal direction of travel take us where we want to go? Are we improving the soil that allows infectious or chronic disease pandemics to seed and proliferate? To answer that, look to our children and ask if they are following us down the hole we have dug for ourselves. The signs sadly say too many are.
By 1987 alarming levels of psychological distress were already affecting young girls: 17% of 15-year-old girls in Scotland. By 2009 the same researcher using the same measures showed that levels had soared to 45% of girls (Sweeting et al, 2009). Between 2009 and 2017, USA adolescents showed a 50% increase in mental health problems (Twenge et al, 2019). The science is now clear that chronic stress negatively impacts health and longevity (Marmot, 2019; Russ et al, 2012), for example by weakening immunity, which is of course relevant to the Covid-19 pandemic. This level of chronic distress has become so widespread that society may even have become inured to it, seeing it as an inevitable ‘norm’. Most adult mental health problems are already established by late teens when around one in four young people have a mental health problem (NHS Digital, 2021). These trends make it clear we are still heading in the wrong direction.
What of our children’s physical health? For example, will they join us in the worldwide diabetes pandemic? Since I became a doctor, diabetes has increased sevenfold in the UK to now affect 7% of us. Many other countries have fared even worse. It is striking that when the rate was 5% it was already using 10% of the NHS budget. This type 2 diabetes is caused by the way we live, yet it is mostly preventable and reversible with lifestyle changes. It used to be seen as a condition of later life, but by 2000 the first UK children with type 2 diabetes were identified (Ehtisham et al, 2004), and some are now coming to amputations even in their 20s. Generational epigenetic changes in DNA (Antoun et al, 2020) may be caused by higher maternal plasma glucose, and in 2015 the first preschool children with type 2 diabetes in Scotland were diagnosed. Our current ways are failing to transform this situation. We won’t get out of this by just working harder at doing what we have always done. To get out of these storms and avoid them in the future, we need to change course.
The living gap: the deep-root cause of our current crises
When we arrive at seeking a new direction, be cautious – it’s an opportune time but also a time vulnerable to us heading enthusiastically off again in a direction that is not grounded in first principles. The compass setting determines the journey. So, initially, reverse the old guidance and don’t just do something – stand there. First attuning to and confronting the predicament – as we have just done with the pandemic soil. Then accepting that’s where we are, seek understanding of the root causes of moving so far off course, and explore what this suffering might be calling for. How are our assumptions no longer serving life?
I believe our era’s crises of health, climate and environment share a common root cause – that’s why they have arisen together. I would call that cause the gap. This gap opens when our wants trump our needs.
More accurately, it’s the gap between our wants and life’s needs. Needs are what must be supplied for life to flourish – everything else is wants. So, let’s call this the living gap. I am using ‘life’ here not in the sense of our life situations or our cultures and their accepted ways of living: I mean ‘life’ as the creative forces that beat our hearts, animates and balances living forms, the planet and its environment and climate. So, in the most straightforward distillation, if a person’s health is not flourishing or a world is not flourishing – it means we are not meeting life’s needs. We may even be sabotaging them. I am not saying that if all life’s needs are met, illness does not happen – rather, where these needs are not met, illness will prosper.
So proposed actions on an individual or scaled-up level need to be tested against core first order principles for wellness: do we have proof that this plan will allow life to thrive; is our compass aligned with life’s needs? We failed to use such principles as we shaped the still-current maps and compass headings that created our industrial revolutions, the rise of consumerism and ultra-processed foods, and the mass release of chemicals into the body of the planet. Thus, the chronic diseases that boomed as the 20th century progressed were seeded long before that. Over 150 years ago John Ruskin warned that our rape of the environment was darkening our skies and damaging the Earth: ‘The light, the air, the waters, all defiled.’ (Ruskin, 1864). By continuing in this direction, this defilement was then extended to our bodies and our children’s bodies – so that by 2018 youths in the USA were getting 67% of their total energy intake from ultra-processed foods (Wang et al, 2021).
If a satnav’s map is wrong, it has to take you to the wrong place. Don’t blame the map: re- programme. Aim to make conscious, and so then examine, the embodied cultural and personal maps that are still drawing us into ever-more dangerous territory. If lost, or in uncharted times and places, a compass is more important than a map – one that aligns with proven first order principles that close the living gap. This will not be the alignment that built the modern world, based on false teaching that represents humankind as individual observers and disconnected entitled manipulators of nature. In reality we are not apart from nature, we are nature.
You are not your mind! You are your ‘true self’ who has a mind
To start closing the living gap, we need to see the mechanisms that drive us personally and collectively to create and follow false compass bearings. Let’s be kind to ourselves here, for so many siren calls pull us off course. We contend with embedded and embodied biological urges and instincts, driven by early-life conditioning and pleasure-addiction circuits, hemmed in by unquestioned (often generational) assumptions and beliefs, and squeezed by cultural and consumer pressures. So, no wonder we are entranced and compelled hypnotically by our wants, even at the expense of life’s true needs. More accurately, this is our ‘mind’s’ wants: that egoic virtual world, that voice-and-picture stream in our heads and its underpinned subconscious mapping and mechanisms. We so easily mistake these thoughts for reality, for ‘facts’, when they are actually made-up hypotheses. If thoughts help life flourish, stick with them, but let’s question them if they don’t. Suffering raises the alarm that our thinking needs to be questioned. A key to unlocking the small mind’s hypnotic power is to ask: who is listening to that voice in our head, that can witness those images, and learn to question them? The fact that we can notice and reflect on these voices, images and emotions, and question them, discloses that there’s more to us, that we don’t have to just blindly believe our thoughts, that we can witness and reflect on them, reshape them. This larger conscious observing presence we could call our ‘true self ’. The unique gift of our time is that perennial wisdom, spiritual practices, and contemporary psychological approaches have all begun to overlap with current sciences, like neurobiology, to understand and cultivate this awareness of the ‘true self ’.
To summarise so far, it’s not personal, but if human drives, born of mind and culture (collective mind), overrule life’s needs, the living gap will open and widen until personal and planetary wellbeing strain, and suffering arises. Ignored, damage follows. The pandemic soil is the inevitable consequence. For humankind to re-align its compass towards life and start again from first principles, we must stop trying to run harder, tracing progress on an obsolete map, and instead change direction. The distress and disorder we experience are guiding lights. By calling for help and pointing to where it is needed, they lead us away from the rocks. But have we learned from our suffering what we must do? To answer that, we need only consider our recent actions, for better and for worse.
The missing side of the health triangle
During the Covid pandemic we heard every day about two appropriate forms of response: prevention and treatment. Current principles of prevention guide us towards vaccination, hygiene measures, social distancing, and lockdowns; our principles of treatment led us to nursing and intensive care, oxygen, then steroids and antivirals. If this prevention and treatment are two sides of a triangle – what might the third side be?
The too-often-missing third side is life’s innate capacity for resistance and recovery, the resilient vitality that underpins the basis of the healing response, growth and flourishing. (Reilly, 2001b). This third side is too often a faint line in the triangle of clinical medicine and public health. It is all but absent in the assumptions underpinning the scientific, medical, and industrial revolutions. The roots of the living gap go deep.
Let’s consider this third side if applied to the spiralling rates of obesity and diabetes. The ‘metabolic syndrome’ drives both conditions, a cluster of changes fuelled by modern lifestyles that generate high background insulin levels (Crofts, 2015). This in turn impairs immunity and boosts inflammatory responses, increasing the risks of many diseases, including more severe Covid. When we measured the fasting insulin levels (which changes long before actual blood sugar levels go too high) of people entering WEL courses in Scotland, almost half of those we sampled were likely or confirmed pre-diabetes (Reilly, 2004–2022). Large population studies, for example in the USA (US Centers for Disease Control and Prevention, 2020) reveal a similar incidence. Dietary changes can correct this core problem – the most fundamental change being a move away from highly processed foods, especially refined sugars. The helpful insulin reduction can then begin within just two days, yet where was this information in the daily government Covid briefings? If only awareness of this third side were more embedded in medicine’s awareness.
The pandemics of non-communicable diseases are not amenable to expert-based ‘fix-it’ medical interventions. To move us away from these lifestyle-driven pandemics of mental unwellness and chronic illness will require radical shifts in our ways of life and thought. With creativity and energy supported by sound policy and proper funding, society could make the change – but don’t wait around for this to happen before you begin to set yourself free, or help others do so, even when still living in adverse situations.
The fifth wave of public health
Over the last 200 years, four waves of public health innovation helped us respond to our medical crises and challenges: sanitation and public works, vaccine and drug development, social innovations like national health services, and identifying risk factors for disease. What we need now is an additional wave, one that’s tuned to and engaged with life’s innate needs and capacities for self regulation and recovery. This fifth wave of public health (Hanlon et al, 2011) would, to use the aphorisms of this article, bridge the living gap, bringing in this missing side of the triangle.
Future infectious pandemics and lifestyle-related pandemics threaten to overwhelm the health services around the world. This is calling for a transformation in ideas about personal and community health. Imagine a fifth wave approach in action. It would lead us to emphasise non-drug methods of tackling the metabolic syndrome; it would ask us to find ways to correct widespread nutritional deficiencies like those of vitamin D and Omega 3 that compromise immunity and inflammatory responses that make many diseases of modernity more likely. Learning from the mass testing for Covid, we might instigate mass testing for these deficiencies and provide supplementation programmes and targeted food cost adjustments. These are just illustrative examples of what embedding the third edge might look like. Be clear, this is a ‘both and’ not an ‘either or’ option, to complement the established prevention and treatment sides of the existing medical triangle.
Life seeds in the dark, the plant wants to grow
Embodied beliefs act as maps, shaping our imagination and perception and in turn how we experience our world and respond to it. So how we perceive the darkness of our current challenges, be they personal or planetary, can pre-set our responses. It is a reflex in us, perhaps from a predator-scanning biological bias, to see the darkness of our suffering and challenges as a threat, an enemy, a dark abyss, which in turn triggers pathways like fear, attack, escape, despair, numbness, and paralysis. It’s natural for a rabbit to freeze in the headlights, but it’s not helpful.
To begin healing, a first principle is to start with an honest acceptance and mapping of the predicament, our current perceptions and experience, our darkness. Indeed, unless we honour this old-current story, any new story will struggle to emerge. We built the search for subsequent change on a foundation of growing safety, trust, and compassionate understanding. Now we can begin to seed hope of shifting from the old story – heroic, but also obsolete and damaging as it is – to become aware of the seeds of hope lying buried in the dark, cold soil of our suffering. Seeds typically need cold and darkness to germinate. If we are alive, they are there, waiting. This is not optimism – ‘it will work out the way I want it to’ – because it might not; this is hope – ‘whatever happens, the strength in me can grow and prevail’.
Wisdom tempers unrealistic hopes, recognising that it is natural to get stressed, ill, suffer, age and eventually die. Yet wisdom says life is robust and has a healing drive. Hope can be based on the solid foundation that life wants out. The seed wants to germinate, the plant wants to grow. We can rely on this. No matter how much life has been suspended, neglected, or abused, when given the right conditions, its innate drive is towards growth, and so healing, wholeness, wellbeing, and joy. We do not have to create these states, but rather help release them in our being, and in larger nature. These states enhance health and wellness, support us if ill, and ease our transition when we are dying.
An icon for these core healing principles is the image below of a beautiful little plant that grew from a seed that waited for 30,000 years in the dark of the permafrost before being given the conditions it needed to germinate (Yashina et al, 2012).
Life responds to nurture: the plant knows how to grow
Let’s look at the seeds of life germinating in us. The following figure shows changes in a group of people on a course structured around these principles. You see in the top half a variety of valuable changes in well-being and self-care, yet some of these areas were not explicitly spelled out in the course. These spontaneous healing shifts illustrate life’s seed in action: when it germinates, life – be it in a plant or in us – knows how to grow; it knows what to do. Our job is to be the gardener, tending the conditions, so that when nurtured life can restore itself, meet challenges and be strengthened by them.
You will see in the lower half of the image the underlying shifts in understanding and fresh perspectives arising through reconnecting to a deeper self, the ‘true self ’: ‘I am not my mind’, ‘I don’t need all the things I thought I did to be happier, healthier or content’, ‘setting aside quiet time each day.’ I believe these words express innate wisdom that is utterly natural, always present, and somehow instinctive within us. They say, ‘give life its chances and the right conditions, and this is what will emerge’. You might hear in them echoes of ancient wisdom traditions. This supports us even when the valuable medical ‘fix-it’ maps are critically needed, but all the more so when no such fix-it is available.
Life-compassion and the nurture principle
My last distilled first order principles relate to how we might release such positive changes by catalysing the underlying innate potentials in life and, consequently, in us. The foundation of recovery and flourishing might be stated as the nurture principle – ‘Life responds to nurture’. This aphorism clarified in the early years of my study of healing encounters. Then, in the search to understand why we fail to nurture our life and treat ourselves so neglectfully, what emerged as a catalysing and central first order principle was compassion, or its lack. The icon graph below shows changes in a measure of self-compassion (Neff, 2003) in a cohort of people before and after attending a WEL course. They showed no change during the three months they waited to join the course, and then on entering the course they showed a progressive and self-sustained rise in measures of self-compassion tracked over the nine months after their course. This graph is stripped of the scientific details to function as an icon that represents the whole study group’s clinically and statistically significant changes, with 57 of the 73 people tracked for 9 months reporting a similar positive shift. These changes correlated with other measures of wellbeing, coping, quality of daily life, and self-care enablement. (Reilly 2014–22, 2013). How did they achieve this?
They experienced a shift during the course that is represented in the next image adjusted by partly eclipsing the word ‘self ’ with a picture of nurture, and then introducing the term ‘life’.
Life-compassion expands us beyond our small ego – the ‘I’ as we usually experience it: ‘what I want’, ‘what I need’, ‘me’, my personality, my story, my past, my future, etc, etc – that entangled maze that leads us to create the living gap. What to do? As Zen says, if you meet a rock, become water. Rather than untangling the mind’s knots, we circumvent this by aiming straight towards activating our deeper basic nurture response. This cross-species instinct is powerful, selfless, tender, fierce and unstoppable. It is pictured throughout our history in our icons of a mother and her infant. However, it’s an odd truth that our nurture response is often more easily activated towards others than towards our troubled self. For example, when we are with a newborn, a seedling, a child, a pet or those who are vulnerable or suffering, a natural response arises that aligns with life’s needs, and evokes caring and respect. We are moved to nurture their life into safety, growth, and flourishing, as the heart opens and expands into affiliative connection to others, even to the Earth itself. So how did these people bring this compassion home to themselves, and how can we?
Here’s a sense of the compassion-activating reflective self-dialogue and images these course participants used to achieve these changes and so begin to bridge their ‘nurture gap’. To get around the rock of the egoic mind, we can use the image of ‘another’. Forget yourself for a moment and imagine a vulnerable life form dependent on you – perhaps a pet, a child, a plant. Now ask yourself: ‘would I treat them the way I treat myself?’ Most of us, most of the time, would not dream of doing to them what we do to ourselves: neglecting core needs, overworking, berating, sleep depriving, and, even if in the name of ‘pleasure’, drugging or addicting, feeding junk food or fluid. We just wouldn’t do it. Let that insight permeate. Now consider: why we would not do this; and why do we neglect and damage ourselves?
Now imagine witnessing an adult mistreating a child or an animal or another adult. Feel the powerful instinctive protective response this invokes. Can you imagine how your life would change if you brought this power to respect your own life, the one that is so dependent on you, the one that is vulnerable to your neglect? The challenge is to bring that same innate compassion to bear on our own life. When someone begins to respect life’s needs and discern them from ‘wants’, wonderful healing things happen. Start with your own life in an act of self-responsibility and self-rescue, rather than a narrow selfishness, and your understanding and care will then naturally expand towards others and out towards the biosphere and the planet.
Recently I tried the same self-compassion measure with a cohort of sixth-year school pupils. Their scores were even worse than the previous adult results. Their results highlighted how low self-compassion strongly correlates with low self-care.
Compassion isn’t a technique. It arises from something deeper and more fundamental at the centre of our being: our capacity for caring and loving kindness. Its absence in the underlying maps used to create our industrialised world had to inevitably lead us into our current unsustainable imbalance in the wellbeing in people, the planet, and all life. It’s time now to rebalance this and bring the profound power of nurturing. This new direction will support life and so let it support us.
I’ll finish with my starting image, which I hope will make more sense now, symbolising some of the first principles we have explored. Life’s potential lies dormant in the seeds, is germinating in the child, and the seedling. Our personal and collective compass at last aligned with life’s needs, the whole is embedded in nature. So, let’s look in this child’s eyes again and let ourselves feel for a moment our caring nurturing instinct.
For further exploration of these ideas
TEDx talk: Unlocking Human Healing
Reilly D (2021) Suffering as a guiding call to change: life-compassion and bridging the living gap. In P Wemyss-Gorman (ed) Innovative approaches to chronic pain. Understanding the experience of pain and suffering and the role of healing. Jessica Kingsley Publishers, pp 63–84.
Reilly D (2017) Don’t fix the dead wood– go for growth. In L Mayes (ed) Beyond the stethoscope: Doctors’ stories of reclaiming hope, heart and healing in medicine. Heart Works Press, pp 53–63.
Conversation with David Reilly and David Peters
Antoun E, Kitaba NT, Titcombe P, Dalrymple KV, Garratt ES, Barton SJ et al (2020) Maternal dysglycaemia, changes in the infant’s epigenome modified with a diet and physical activity intervention in pregnancy: Secondary analysis of a randomised control trial. PLOS Medicine, 17(11) e1003229.
Crofts CAP, Zinn C, Wheldon M & Schofield G (2015) Hyperinsulinemia: A unifying theory of chronic disease? Diabesity, 1(4) 34–43.
Ehtisham S, Hattersley AT, Dunger DB & Barrett TG (2004) British Society for Paediatric Endocrinology and Diabetes Clinical Trials Group. First UK survey of paediatric type 2 diabetes and MODY. Archives of Disease in Childhood, 89, 526–529. http://dx.doi.org/10.1136/adc.2003.027821
Hanlon P, Carlisle S, Hannah M, Reilly D & Lyon A (2011) Making the case for a ‘fifth wave’ in public health. Public Health, 125, 30–6.
Kompaniyets L, Goodman AB, Belay B et al (2021) Body mass index and risk for Covid-19–related hospitalization, intensive care unit admission, invasive mechanical ventilation, and death – United States, March–December 2020. Morbidity and Mortality Weekly Report (MMWR) 70(10) 355–361.
Marmot M (2019) A health crisis is a social crisis. BMJ, 365, l2278.
Mercer SW, Watt GC & Reilly D (2001) Empathy is important for enablement. BMJ, 322, 865.
Neff KD (2003) Development and validation of a scale to measure self-compassion. Self and Identity, 2, 223–250.
NHS Digital (2021) Mental health of children and young people in England 2021 – wave 2 follow up to the 2017 survey. (accessed 6 May 2002).
Reilly D (2013) The healing shift enquiry – creating a shift in healthcare. Journal of Holistic Healthcare, 10(1) 9–14.
Reilly D 2004–2022. TheWEL: The Wellness Enhancement Learning Programme. TheWELworld.org.
Reilly D (2001a) Creative consulting – you can make a difference. BMJ, 323, 0109309.
Reilly D (2001b) Enhancing human healing. BMJ, 322, 120–1.
Richardson S, Hirsch JS, Narasimhan M, Crawford JM, McGinn T, Davidson KW et al (2020) Presenting characteristics, comorbidities, and outcomes among 5700 patients hospitalized with COVID-19 in the New York City area. JAMA, 323(20) 2052–2059.
Ruskin J (1864) The queen of the air – being a study of the Greek myths of cloud and storm [Online] (Accessed 9 May 2022).
Russ TC, Stamatakis E, Hamer M, Starr JM, Kivimäki M & Batty GD (2012) Association between psychological distress and mortality: individual participant pooled analysis of 10 prospective cohort studies. BMJ, 345.
Sweeting H, Young R & West P (2009) GHQ increases among Scottish 15-year-olds 1987–2006. Soc Psychiatry Psychiatr Epidemiol, 44, 579–86.
Twenge JM, Cooper AB, Joiner TE, Duffy ME & Binau SG (2019) Age, period, and cohort trends in mood disorder indicators and suiciderelated outcomes in a nationally representative dataset, 2005–2017. Journal of Abnormal Psychology, 128, 185–199.
US Centers for Disease Control and Prevention (2020) National diabetes statistics report, 2020. US Department of Health and Human Services.
Wang L, Martínez Steele E, Du M, Pomeranz JL, O’Connor LE, Herrick KA, Luo H, Zhang X, Mozaffarian D & Zhang FF (2021) Trends in consumption of ultraprocessed foods among US youths aged 2–19 Years, 1999–2018. JAMA, 326, 519–530.
Yashina S, Gubin S, Maksimovich S, Yashina A, Gakhova E & Gilichinsky D (2012) Regeneration of whole fertile plants from 30,000-y-old fruit tissue buried in Siberian permafrost. Proc Natl Acad Sci USA, 109, 4008–13.






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}