

Painting the doctor– patient relationship
Inova Shun Wah Lee, Medical student, Barts and The London School of Medicine and Dentistry
Published in JHH18.1 – Flourishing in Medical Education
My interest in medicine stemmed from growing up with a special needs sister with Williams Syndrome, who needed numerous operations and multi-disciplinary care. Both of us also grew up surrounded by music and a strong interest in art, which have become some of the ways for us to communicate and enjoy each other’s company. Since coming to medical school, the opportunity in our first year to undertake the student selected component (SSC) exploring creative arts in health and illness really helped me realise how to amalgamate the two worlds of medicine and the arts. Currently, I am intercalating in Prehospital Medicine iBSc having done three years of medicine and, during this time, I’ve seen the benefits of this integration, especially in my reflective practice. My learning in anatomy has also been enriched with opportunities like the anatomical art SSC. Additionally, I’ve been able to produce a children’s comic for the Centre for Trauma Sciences in The Royal London Hospital to teach children about the research and management of bleeding and clotting. I have found that embracing this creative way of thinking has made academic and clinical experiences even more meaningful, which I hope to translate to clinical practice as a doctor.
Introduction
It is a familiar concept that we should ‘treat the patient, not just the disease’ (Spaeth, 2015). To achieve this, I used to think that the narrative and emotional expression was confined to a one-way flow from patient to doctor. But the notion that ‘the clinician must not only see, but be seen’ (DasGupta, 2008) gives a whole new dimension to the doctor–patient relationship. The patient’s story and best course of care are more likely to emerge when both parties share their humanity.
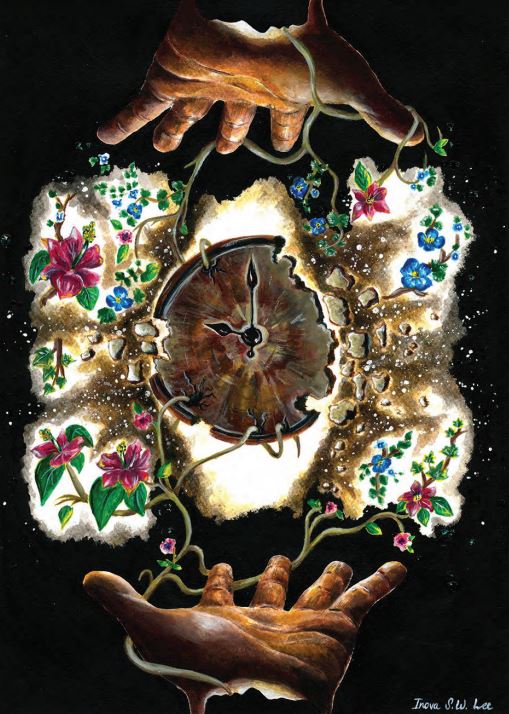
As a reflection, I produced this painting on my exploration of the doctor–patient relationship.
Mutuality
There are two hands, one representing the doctor and the other the patient. Their alikeness portrays how both parties share the same human vulnerabilities and emotions. The open hands not only convey the patient reaching out for medical help and the doctor offering it, but also the giving and receiving of one another’s narratives. Hearing a patient’s story can be a moving experience and these emotions don’t always need to be hidden. They can help both people to connect on a human level. The silhouetted faces represent patient confidentiality. The doctor and patient can ‘see’ each other but are anonymous to any outsiders. It is not obvious which face represents which person, dismissing any hierarchy between them. I have met many patients who were experts in their illness. Approaching their story with humility made me more receptive and able to understand them.
Communication
In the painting, a stem arises from each mouth and branches out, symbolising the different forms of communication. To have one’s story listened to and accepted can be incredibly empowering and validating. When communication blossoms (ie the flowers) then respect, trust and the determination to reach a common goal follows. Crucially, the doctor’s choice of words can be ‘gate-openers or gate-slammers’ to new strands of the patient’s story (Cousins, 1982). And I have realised that history-taking is a conversation, rather than an interview. There needs to be a crossover into the patient’s language, in the same way that the different coloured flowers mix in the painting.
Inevitably, some barriers will be present, particularly time limitations. The central clock in the painting keeps the hands apart. However, as it cracks, the specks dissolve into water droplets that feed the plants around it. This represents how the release from time constraints can help the doctor–patient relationship grow, as patients often open up when given the time and space to do so. The branches curled through the clock acknowledge that time constraints are ever-present. But I have found that openness about this encourages an effort to work around that together.
Perspective
The painting can be viewed from any orientation. As you rotate it, the different story you see reflects the flexibility and empathy we need, although we can never fully know another’s experience (DasGupta, 2008). I have also learnt that trying a new angle or asking a question differently can uncover new details. When the painting is turned horizontally, the features form an eye. We all have our way of seeing things and unique experiences. So in the doctor–patient relationship, our differing perspectives will impact how well we understand each other. It is important to acknowledge this and understand how our assumptions influence the way care is provided.
To conclude, a successful doctor–patient relationship has many elements including respect, trust and an open, honest expression of each individual’s story. If we want to keep care patient-centred, we should not view our own humanity as a hindrance. In fact, sharing it may help the patient reveal more of their own narrative, under the safety net of patient confidentiality. By embracing these elements, doctor–patient relationships can thrive.
References
- Cousins N (1982) The physician as communicator. JAMA, 248(5) 587–589.
- DasGupta S (2008) Narrative humility. The Lancet, 371(9617) 980–981. Spaeth GL (2015) Treat the patient – not just the disease. www.reviewofophthalmology.com/article/treat-the-patient-not-just-the[1]disease (accessed 18 February 2021).






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}