
Do we doctors underestimate our patients’ interest in lifestyle change and willingness to collaborate to improve health?
David Unwin, GP; RCGP National Champion for Collaborative Care and Support Planning in Obesity & Diabetes RCGP clinical expert in diabetes
Published in JHH13.2 – Nutrition and Lifestyle
A GP partner in Southport for 30 years, I have witnessed first-hand the twin epidemics of sugar (type 2) diabetes and obesity developing in my community. Also I noticed I was spending more and more time signing prescriptions, monitoring blood tests and checking blood pressure. Deep down there was a nagging doubt about this being the best use of my time and energy to help my patients find good health.The results just didn’t seem that good. I began to have success in getting patients to give up sugar completely and the rest is history!
Yesterday I asked a patient how she felt about being on long-term medication for her blood pressure.
‘It’s a worry as I’m only 40 and it’s taking three different meds to keep my BP down, also how many can you keep adding and be safe?’
This presented the ideal opportunity to explore lifestyle improvements as an adjunct to her care. She said it was a ‘relief’ to feel she might be able to ‘take control’. To my embarrassment she had not been weighed for some years, so we agreed to get a baseline weight measurements (96kg) and added in a waist circumference (118 cm); she was surprised to hear weight loss would really help her case and may even give her the chance of reducing medication.
For the past four years I have been experimenting with a lower carbohydrate diet to help interested patients like this one. I keep an Excel spreadsheet of anonymised (and consented) patients as a rather lowbrow basis to my practice-based research (Unwin and Unwin 2014; Unwin and Tobin 2015; Unwin 2014a; Unwin et al 2015). So I can tell you I now have a case series of 91 patients on the diet for an average of 15 months who have lost an average of 8.8 kilos. Over 40 of my patients weigh less now than at any time since the year 2000!
In my case series the systolic BP drops by an average of 7.5mmHg, the diastolic by 5.5mmHg, giving me hope for the lady from yesterday. But quite unlike most drugs which only target a single surrogate marker she may experience a whole host of other improvements. The average cholesterol drops by 0.36, and the cholesterol ratio by 0.47. Of the 91 low-carb cases, 60 have diabetes and the average HbA1c dropped by an amazing 12.1 mmol/mol taking many into the pre-diabetes category and avoiding metformin. Added to this are reported improvements that cannot be measured; self-esteem, knee and back pain, more energy and feeling younger.
Results I was quite unable to achieve in the first 25 years in practice. I wonder why?
I suspect it’s a question of belief. At medical school we spent months learning pharmacology as ‘the most important tool of our trade’ alongside surgery. Lifestyle medicine and even disease prevention was hardly given a mention, it just wasn’t sexy. Also medicine was something ‘done to patients’ whose part was to get better and be grateful! This situation was compounded by ‘evidence based medicine’ where the drug companies were very quick to see the advantages of funding research, but who would pay for studies into diet or exercise? Relatively very few. Another problem – the gold standard of evidence based medicine is the randomised controlled study. Drugs can be ‘placebo’ or ‘active ingredient’ but without resorting to naso – gastric feeding folk obviously know what they just ate. On top of this is the problem of diet standardisation; if you give 100 people a diet sheet and advice you will get very different interpretations of your diet, and on top of that is the problem of recalling what you eat accurately, possibly for years. So I do have some sympathy with those who prefer to stick with drug trials, but arguably we now have a skewed evidence base. For years I was bombarded with ‘evidence’ by the drug reps and made to feel old- fashioned and out of touch if I didn’t ‘keep up’ by prescribing their products.
Light dawned with asking WHY the patient is unwell (causation)
Very gradually I began to have a vague sense of failure, signing literally hundreds of scrips for folk who didn’t really seem much better, spending ages measuring BPs and adding in more medication. Then the depressing business of the guidelines – many of my patients have multiple problems – so which to prioritise; diabetes, hypertension, obesity, depression or osteopenia? Also the patients didn’t seem to shine with health no matter how many medications I gave them, nor were they very interested or grateful! It occurred to me one day that a person weighing 18 stone with central obesity, knee pain and dyspnoea isn’t a well person no matter how many drugs I use. I had stopped asking WHY my patient was ill, what were the true causes of the illnesses I was dealing with? Hypertension, diabetes, obesity, chronic pain, even depression? Instead I was substituting what would satisfy them, so I could rush on to the next case. The focus of my consultations had become ‘can I either reassure it’s trivial, prescribe a drug or refer onto a specialist?’ Even a lot of the tests I arranged related to these activities.
Looking back it was the rarity of using my skills to cure patients that was feeding that sense of failure.
Essential hypertension illustrates my point. Four years ago at a clinical meeting I asked the question What is the cause of essential hypertension? Mystified that I should even ask colleagues explained patiently ‘that’s why it’s called “essential” – we don’t know’. I replied, ‘If you don’t know the cause how can you be sure what the best treatment is?’ In the end it was agreed I thought too much and we should just follow the guidelines! Around the same time in one week I called out three ambulances for elderly people who collapsed in hot weather due to overtreatment with anti-hypertensive drugs. There had to be another way. I started incorporating more lifestyle advice into the consultation, particularly before initiating lifelong medication (Unwin 2014b). I made an exciting discovery: given a choice many patients appreciate the chance to take control of their health by losing weight or taking more exercise as an alternative to drugs. So now for moderate hypertension, instead of prescribing straight off I might offer the patient these alternatives as a trial for say a month. First establishing a baseline weight, sometimes lending them a BP machine to facilitate feedback. A hint; instead of being too prescriptive about exercise it helps to ask ‘if you were to do more exercise what would suit you best?’ Also at review be sure to ask how this is going as it’s a chance for positive feedback.
Type 2 diabetes is another condition that rewards more thought around causation and patient empowerment.
After I joined my GP practice in 1986 we did a survey of our patients with type 2 diabetes. There were just 57 cases in a practice of 9,000. In ‘the olden days’ we called this either ‘sugar diabetes’ or ‘maturity onset diabetes’ to reflect the facts that it usually developed first in the mid-60s or later, and that sugar was agreed to be part of its causation. At that time we had no patients with type 2 diabetes under the age of 50. Now, 30 years on, we have 21 patients under 50 (whose average body weight is a worrying 17.5 stones). The youngest is 34. I have seen greater than a six-fold increase in prevalence of diagnosed diabetes with well over 400 patients now having type 2 diabetes! Something has changed; it cannot be my patients’ genes, only a changed environment acting upon a genetic predisposition can account for it. Four years ago I had no idea why this was, or that anything could be done to halt the associated epidemic of obesity that was so obvious, and in younger and younger patients too.
called this either ‘sugar diabetes’ or ‘maturity onset diabetes’ to reflect the facts that it usually developed first in the mid-60s or later, and that sugar was agreed to be part of its causation. At that time we had no patients with type 2 diabetes under the age of 50. Now, 30 years on, we have 21 patients under 50 (whose average body weight is a worrying 17.5 stones). The youngest is 34. I have seen greater than a six-fold increase in prevalence of diagnosed diabetes with well over 400 patients now having type 2 diabetes! Something has changed; it cannot be my patients’ genes, only a changed environment acting upon a genetic predisposition can account for it. Four years ago I had no idea why this was, or that anything could be done to halt the associated epidemic of obesity that was so obvious, and in younger and younger patients too.
I mentioned earlier the role that belief in lifestyle inter – ventions has had in improving my effectiveness as a GP. Nothing illustrates this better than diabetes. Before, although I referred my patients on to a dietician, it wasn’t done with any conviction that diet could make much difference. But what a difference it made once I had reconnected with the idea that dietary sugar was obviously a huge part in the causation of this miserable epidemic. I added in another discovery about the huge amount of blood glucose liberated by the digestion of starchy foods like bread or rice. Now I had a model of causation I really believed in: sugar and refined carbohydrates were the ‘cause’.
Again, when I asked my patients I found they were really interested in avoiding drugs like metformin and were quite prepared to make changes, particularly since my early cases had shown me the huge difference that giving up sugar and starchy foods could make (Unwin and Unwin, 2014).
I came across this quote in a health professional blog recently:
‘I continue to be worried about how the term lifestyle medicine is used to exacerbate the victim-blaming that is endemic within our society.
I have worried about this too. It’s possible that instead of dealing with the many health inequalities that exist in society we may just blame our patients for not ‘getting a grip’. If I’m really honest when I was young, fit, and slim, this was exacerbated by nasty undertones around ‘lack of willpower’ which I suspected was often a factor. Since then, age and a clinical psychologist wife have taught me a lot about behaviour change, and the benefits of getting relationships to a more adult-adult state
For me sometimes it helps to start with the patient’s own goals (not my goals for them). For example to have more energy, to come off drugs or to look more attractive.
 Then supply tailored information, not advice (which has tones of obligation and is schoolmasterly). For example a single small slice of wholemeal bread has the same effect on your blood sugar as three teaspoons of table sugar. A bowl of rice is equivalent to ten teaspoons of sugar, a small baked potato eight. For someone with diabetes this information is useful in shaping their dietary choices.
Then supply tailored information, not advice (which has tones of obligation and is schoolmasterly). For example a single small slice of wholemeal bread has the same effect on your blood sugar as three teaspoons of table sugar. A bowl of rice is equivalent to ten teaspoons of sugar, a small baked potato eight. For someone with diabetes this information is useful in shaping their dietary choices.
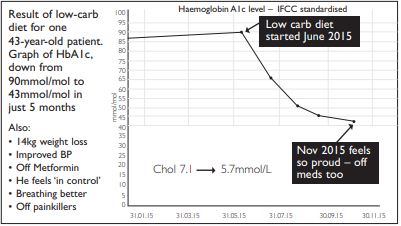
Follow up with ongoing support and feedback. My psychologist wife reminds me how important feedback is to behavioural change. The Emis GP computer system generates graphs very easily (see the two examples of patients’ progress above). Patients are delighted to take them home to prove to the family how they are doing.
Of course it’s not always good news. So often after Christmas or a holiday there is a disappointing weight gain. I have learnt not to be unhappy at this but see it as an opportunity for reflection. Try asking what have you learnt from this that you would do differently next year?
Golden opportunities
As with any relationship picking the best time to make a suggestion to our patients is very important. When are we most likely to be listened to? I would suggest it’s when there is a sudden change in the course of someone’s case. The moment we inform a patient they are hypertensive, diabetic or pre-diabetic, alarm bells are ringing about possible future consequences and so there is far greater attention paid to any information we supply. Similarly when someone previously stable needs an increase in medication there is a sense of slight danger, because most folk are not delighted to take medication and I have found them very open to alternative approaches.
Now as I look actively for these golden opportunities, the list of them is growing all the time but for the present I would suggest anyone with central obesity who also has:
- a new diagnosis of diabetes or pre-diabetes
- an abnormal blood pressure result
- mild to moderate arthritis of the knees
- abnormal liver function (Unwin et al, 2015) (but denying abnormal alcohol intake and not on enzyme-changing drugs)
I feel general practice is an ideal medium for this approach because of the continuity and mutual trust we have with our patients. Collaborating with patients can be so cheerful and fulfilling. Now at the end of my career I feel I am starting to be a proper doctor at last!
References
- Unwin DJ (2014a) Diabesity: Perhaps we can make a difference after all? Diabesity in Practice 3(4) pp 131-134. Available at: www.diabesity-co.uk/media/content/_master/3963/files/pdf/dip3-4-131-4.pdf (accessed 30 August 2016).
- Unwin DJ, Cuthbertson DJ, Feinman R, Sprung VS (2015) Raised GGT levels, Diabetes and NAFLD: Is dietary carbohydrate a link? Primary care pilot of a low carbohydrate diet. Diabesity in Practice. Available at: http://bit.ly/1NYsS6x (accessed 30 August 2016).
- Unwin DJ, Tobin SM (2015) A patient request for some ‘deprescribing’. BMJ 351. doi: http://dx.doi.org/10.1136/bmj.h4023.
- Unwin D, Unwin J (2014) Low carbohydrate diet to achieve weight loss and improve HbA1c in type 2 diabetes and pre diabetes: experience from one general practice. Practical Diabetes 31(2) pp 76. Available at: http://onlinelibrary.wiley.com/doi/10.1002/pdi.1835/abstract (accessed 30 August 2016).






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}