
Darkness, life-compassion and the seeds of transformation- Notes and results from the front line of The Healing Shift Enquiry
David Reilly, Director,TheWEL programmes and The Healing Shift Enquiry
Published in JHH15.1 – Transformative innovation in healthcare
I’ve centred the four decades of my career as a doctor on studying our life’s ability to heal itself. I remain a student.These notes are a work in progress.
Impacted by its over mechanised ways, I almost left medical school in fourth year, but I stayed on vowing to be part of change – at least within myself. And I had a dream that one day we would talk not just about diseases and treatments, but about our human healing capacity – and that this would create a different focus for the world of medicine and health.This focus has now been posited as the basis of a new ‘fifth wave’ of public health.
But be it in me or you, dreams are not enough, and caution is needed to not just shoot off after a ‘good idea’ without clear evidence – or another dead-end wave is generated. A new vision – a ‘third horizon’* – must be rooted in first-principle evidence of clear effect, proof that this path leads to real transformation.That’s the path that calls me.
[bctt tweet=”When the shift happens and the seed germinates the effects ring through the whole organism” username=”BritishHolistic”] The blank slide: darkness
Can I begin with my most important image. See Figure 1
 It’s a blank. What do you see when you look into, not at, this darkness? If this is the darkness in your own life, what do you see, how do you react as you look into it? A common perception is a form of abyss, or a trap. What feelings does this raise in you? For many it may be stuff like fear, despair, entrapment, hopelessness. Many of us have had such dark experiences, and some never return.
It’s a blank. What do you see when you look into, not at, this darkness? If this is the darkness in your own life, what do you see, how do you react as you look into it? A common perception is a form of abyss, or a trap. What feelings does this raise in you? For many it may be stuff like fear, despair, entrapment, hopelessness. Many of us have had such dark experiences, and some never return.
Now swap the image. What if you see this darkness as an enemy? This is the way we often see our diseases, or our suffering, or lack of wellbeing. What state does that image generate in you? How does your body feel as it meets this enemy? Making ready to fight, warfare? How does this differ from the abyss?
Let’s change the image once more. What if this is a blank canvas in a dark room, waiting for the light of dawn, and the creation of a new image? Do you feel the difference within you?
Your physiology, and so your health and wellbeing, follows as the servant of these image-generated states – created by your shift in interpretive (if often reflex) perception of the very same darkness. In rats injected with tumour and then subjected to electric shocks, ‘only 27% of the rats receiving inescapable shock rejected the tumor whereas 63% of the rats receiving escapable shock and 54% of the rats receiving no shock rejected the tumor’ (Visintainer et al, 1982). This is how a state of helplessness contrasts with one of empowerment. A sense of travelling a road out of darkness seems to enhance health even more than dark’s absence.
The seed
I now see the darkness of human suffering as soil, soil containing seeds waiting to germinate. So viewed, the world is different. So viewed, the work to be done spontaneously reshapes. The dark and the cold are the very things that seeds need to germinate. Our suffering, our darkness, primes us for transformation, and calls out strengths that would otherwise remain dormant. So viewed, suffering is not the enemy. It is seen as the precondition, and the call for change – from the friend of our life. It’s normal to suffer – as it is to age, get sick and die. That’s why we need compassion as our deeper response to the human predicament.
The gardener
So – what now? I think we need to study gardening – human gardening.
In 2012 Russian scientists reported that they had germinated seeds found in the Siberian permafrost, buried by an ice-age squirrel over 30,000 years ago. Later they blossomed with a unique form to their flowers (see Figure 2). (Yashina et al, 2012).
Life wants out. It awaits the conditions, then it will emerge. It does not argue or resist. Sometimes it can repair the body, at times it can restore spirit. This universally applicable truth is powerful knowledge for someone who is labouring under the burden of suffering or illness. It is a powerful foundation for planning human caring and endeavour.
Mapping the human healing response
If you stress or damage an organism its inherent drive is to bounce back, or if overwhelmed, go to seed. We need a direct study of this ‘healing response’ in humans (Reilly, 2001). Let’s be curious about this capacity for growth and healing, and consider the conditions that block it or help set it free. Perhaps growth, healing, and creativity are water we can draw from the same well. To study healing is not to measure an object, it is an inherent drive, but its behaviours and fruits can be readily mapped.
There’s something unconditionally generous about life’s processes. If a plant has drooping leaves, and you water it after a period of neglect, it doesn’t object, it responds. How come? As I shifted from a map dominated by bringing ‘interventions’ and treatments, to one that worked to release inherent strength – the results transformed. And I transformed – from Descarte’s apprentice watch repairer, into a student of human gardening.
Life heals. You cut yourself, it heals; you break your heart, it works to reclaim your wholeness; a whole continent is devastated: one hundred million people killed in 20th century wars and yet there’s an unstoppable movement back towards order and peace. So when I use the word ‘life’ here, I don’t mean the life situations we all have – they just cycle: if it’s up it will be going down, and if it’s down, and you hold out through the storm, it will be back up one day. No, what I am calling life here is that which beats your heart. This life is the carer’s greatest ally, the suffering person’s hope.
Who knows what life ‘is’? Our science can study, describe, define, discern mechanisms and manipulate it – but we still don’t know what it is. Fortunately, plants know how to grow. Gardeners don’t make the plant grow, and don’t have to know how it grows, they just learn how to support it. In the pain clinic where I worked for 10 years seeing people the clinic had failed to help, eventually the only prerequisite clinical sign I sought was that my patient’s heart was beating. That was enough. Because life wants out, it wants to be free. Life is stronger and bigger than we are. So, in a sense, learning not to take one’s suffering and recovery personally can be very helpful. Don’t take yourself so personally. Take care of your life. Just these perceptions in themselves proved to be a medicine – before any dialogue or work took place.
Our predicament – our first horizon – our epidemics
Why bother with all this? If the ‘plant’ of your life is struggling, you are not alone. Post-industrial societies are struggling. Our children are succumbing earlier and earlier to the new epidemics. A young girl in Scotland now has more than a 40% chance of significant psychological distress by the age of 15 (Sweeting et al, 2009). And the science is now clear that chronic distress translates into more disease and earlier death (Russ et al, 2012). Children born in the century before 1970 had a 2–3% chance of becoming obese adults – this has since increased tenfold (Harcombe, 2010). Life-style related diabetes now affect 1 in 11 of humanity and 5–7% of the UK – and even at 5% this is using up 10% of the whole NHS budget (www.diabetes.co.uk/cost-of-diabetes.html). And it is going to get worse. It is now being diagnosed in primary schools, and in preschool children tipping dialogue into terms of ‘tragedy’ and ‘disaster’ (Diabetes.co.uk, 2015). Some affected as teenagers are coming to their amputations in their 20s. It’s already worse in other parts of the world – for example, in Qatar the type II diabetes rate is 26%.
Note that many degenerative diseases and cancers are happening younger and younger – which belies talk of the epidemics being a result of ‘medical success’ of people living longer. It seems we – public, patients, staff, policymakers – don’t adequately understand how to flourish in the modern world. So we lean more heavily on our old maps, increasing our prescribing, extending our waiting times. We are improving management of course: by harder work, better targets, better drugs, efficiency measures – but, this is not transforming our predicament, only containing, mitigating, palliating this darkness.
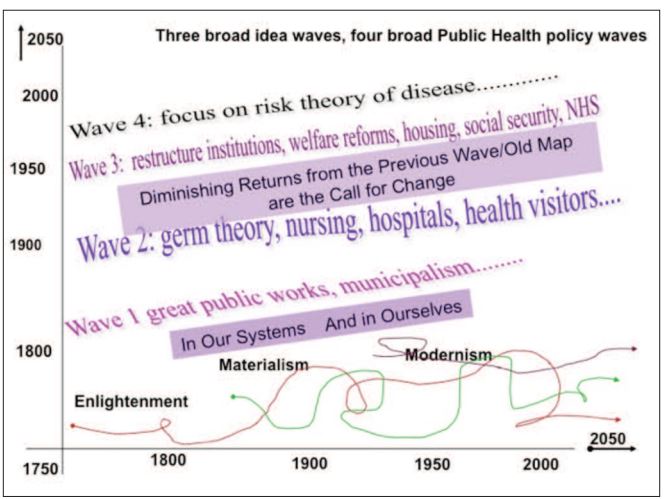
Our interventions, based on the four great waves of public health of the last two centuries (Figure 3), are now delivering diminishing returns.
Personally or collectively, our old maps ‘worked’ for us in another time – and so we may cling to them even when times have changed. On a larger scale, our maps built empires, industrial revolutions, the modern world – no wonder we believe them now even as we hit the impasse. At their core these four waves rely on experts and their powers to intervene. Now these ‘fix-it’ ways are not working in the modern epidemics – you can’t just ‘fix’ diabetes, anxiety, depression, obesity, chronic pain, chronic inflammation, chronic fatigue, and more. We need a new wave of innovation, and a new guiding map for a change of era (Reilly, 2013b; Hanlon et al, 2011a, 2011b, 2012).
Do we see this yet? Do we ‘get’ it yet? We have many ways to defend our old maps, and use up a mass of resources and human endeavour and care trying to hold up that first horizon. Currently around 40% of the population have long-term conditions. What will be the tipping point till it is common understanding that drugs and surgery and stern words are not enough – for a person in pain, for a people in pain.
The journey of change
Yet, here, trapped in the darkness of our First Horizon, with so many heroically ‘keeping the lights on’, it’s hard to see that our maps, our thinking and structures won’t free us. Often we keep going in our lives pushing harder through our predicament, our suffering – until we break down. That, as that old but still true cliché says, is often the point of breakthrough. So, truth is, the sooner we have our breakdowns the better… then the cry is heard – calling for that third horizon, that different way, and so leading us into our next cycle of the ‘hero’s journey’ of change. This sequence, this pattern in human affairs, is like a fractal, it is ‘scale independent’ – it applies in our personal world, or our collective world. As carers – of ourselves and others – coming to understand these components of a journey of change is critically helpful.
But where to begin? It must be from right here. When overwhelmed our imagination can freeze – and we can’t see a road out to freedom. First, we need to know, to remember, or be reminded, that healing is possible and waiting. Then, we look for inspiration, real examples of successful changes, however small-scale. We breath that in – inspire – and we are sparked, catalysed, germinated. Let’s look at inspirational transformation in action in other epidemics – in Glasgow in the 19th century. More than 10,000 people died in that city as the periodic cholera swept through. Contemporary care palliated, but could did not stop the onslaught. Then, someone dreamt of change. They envisaged bringing a clean water supply into the city. How do we respond to dreamers when they describe a new horizon to us, as we tackle our predicaments in what we tell them is ‘the real world’? The idea was rejected for years by many people including those with vested interests like water companies, landowners and even the admiralty: it would ‘bankrupt us, poison us, can’t be done, it won’t work, it’s technically too difficult…’. Note today’s parallels here to big business conflicts over ‘clean food’ rather than clean water. Sometimes darkness has to deepen before we are able to really question our current maps and envisage our release. It took decades of controversy before the clean water of Loch Katrine flowed into the city from a project as ambitious in its day as the moon landing. In the 1866 epidemic Glasgow escaped almost unscathed, with only 53 deaths compared with more than 4,000 in the 1848–49 epidemic (BBC, 2014; McCombes, 2010).
Today analogous epidemics are killing more than cholera ever did. Can we dream a world where our children will be spared in today’s epidemics? If not, we are trapped in the darkness by our own poverty of vision. What would be our equivalent ‘clean water’ to transform our current populations health? That was the quest behind the Fifth Wave of Public Health project and the AfterNow work it spawned. Your dream may be critical to us.
The shift
Maybe each generation is called afresh to learn about these cycles of darkness and response. We are left clues and buried maps by our predecessors in the substance of much of our narratives, myths and stories, and our wisdom traditions – as explored so well for us by Joseph Campbell (Campbell, 2008). But these words of guidance, their framing, may fail to transmit these truths adequately to a new generation. I dare to wonder if a focus on engaging with healing capacity was placed more centrally in our learning, our science, its generational transmission would strengthen.
The journey of change builds on our awareness of where we are – and so any suffering needs acknowledging not diverted, drugged, distracted. Acceptance deepens – it is how it is, not as we would wish it to be. This is not resignation, it is honest turning towards the pain. We come to see our suffering as a call of change and not an enemy. We realise that the diminishing returns of our current ways (H1) are signs that the future cannot be only be based on the maps that built our current world view. We get beyond attacking the old maps – recognising ways they were effective in their day, keeping what is good still.
We seek the core understanding that will build the new maps we need. These foundations make us ready, primed, to find inspiration and so rediscover our inherent hope. With such activation comes action.
A caution: as we explore new ways, we often must walk off the confines of the current evidence-based maps – so we need be wary of firing off second horizon innovations that lack practice-based proof of transformative effect. People in need are vulnerable – they may buy any promise of a ‘quick fix’. Fashion is everywhere, even if the clothes are intellectual or managerial, or whatever. Much personal or large scale ‘innovation’ ends up being about doing the old better map, propping up old ways, rather than charting a better new path.
What direction to travel? I found to avoid a wasted journey, return to a core principle: point the compass at life itself. Ask ‘does this create the conditions that allow life to emerge, does this serve life?’. If it does, and you improve the gardening, something creative, something healing will happen. You won’t know what it’s going to be – and be ready for it not corresponding to your five-year goal, your target weight or your academic or financial dreams. This not-knowing is called adventure.
To explore this for yourself, or with others, maybe try the following reflective enquiry. It’s a simple sequence I’ve found can catalyse perceptual shift, and so generate new maps. It uses images to circumvent the current maps and egoic-self. At its core is an activation of a change of heart – and this is aided by using images of dependent life in need of care – like a plant, a child, a pet.
Life-compassion dialogue
Taking account of any suffering or strain… eyes closed if this helps, in a quiet reflective way – let an image or idea come in response to these questions:
‘If you were plant what shape are you in?’
Let an image come to mind that reflects this and take notice.
Now ask: ‘What does this plant need, what is it calling for?
Let a quiet voice or a feeling come through. If it comes in metaphor – like ‘light’ or ‘water’… then ask what that would be at a practical level in my life, my day to day living.
Now, sitting with this image of your life; ask…
‘Whose plant it? Who is responsible for it? Who is the gardener?’
Yes, only you. It’s no one else’s job. No one else can do this for you, eat for you, sleep for you, nurture your life…
Give yourself a score out of 10 for your self-gardening. Could it be better?
The healing shift enquiry
I became a student of survival; then of recovery; then of flourishing. As I discovered the limits of current orthodoxy, I also found that complementary medicine is not it – it lacks awareness of public health and is still basically an expert/fix-it model. Both systems have value, neither are providing the transformative components we need to face our chronic disease epidemics. I came to stop looking for treatment systems and adopted ‘first principle’ working. My clinical field studies involved working with people who had experienced recovery either through their own efforts, and/or through any effects of our consultations together. I studied this with them directly, working outwards from there, ‘reverse engineering’. Avoiding ideas, fantasies, speculation, theory, philosophy as best I could, I tried to understand something of how these people had survived. Sometimes I’d ask ‘How come you’re not dead?’ It’s a provocative question, so be sensitive about the timing! But at the right moment it can reveal a lot about what has been keeping them going and how they had got through. I’d also ask for their teaching if something we had done together was effective. I was also learning from my own life and the people close to me.
As I watched people recover and transform their lives in the middle of the epidemics, they were like poppies on a battlefield and somehow I felt they were holding answers, if only I could hear them well enough. I remember one of my formative conversations with a woman in the early 1980s – it held the essence that would later seed the ‘fifth wave’ ideas. We held a first consultation together in the pain clinic. She had run the gamut of drugs and procedures but was still struggling. She was wondering about the gamut of alternative medicine. We were exploring my nascent efforts at what I’d later call a therapeutic consultation. At the end of what I knew to be an important meeting for her, I asked her: ‘In view of our meeting, how would you feel if I didn’t prescribe anything?’ It seems simple now, but then it ran counter to my training and medicine’s maps to ‘do something’. She was delighted. ‘That would be great, people just seem to always want to do things to me, or have me take drugs.’
When she came back four weeks later, she described a transformative experience to me. She was different. There were radical shifts in her whole health, her whole world, her whole wellbeing. In addition, the negative impact of her pain was meaningfully reduced.
I realised that if I had prescribed something (orthodox or otherwise), she and I would be having a conversation about what a fantastic medicine that was, and I’d be asking the kind of questions practitioners ask about – how quickly it had acted, what had the treatment done at first, how it developed then, and had it worn off yet, and should we repeat it: a health intervention conversation that has been repeated billions of times around the planet. She helped move me off this territory, to accept that this outcome was entirely due to what had happened between us – and thus within her. I had seen this ‘healing response’ as I called it before, but always interwoven with and so attributed to an intervention or its placebo effect. Now I had to confront this capacity directly, creatively. In studying this I could refocus and supplement the usual practitioner’s questions unfettered. I could ask, ‘Did you know you had this in you? How did you achieve this?’ (Note the empowering new anchors this brings). ‘Why do you think this happened; why did it not happen before; was there anything that we did that helped? What does it need now?’ And so on.
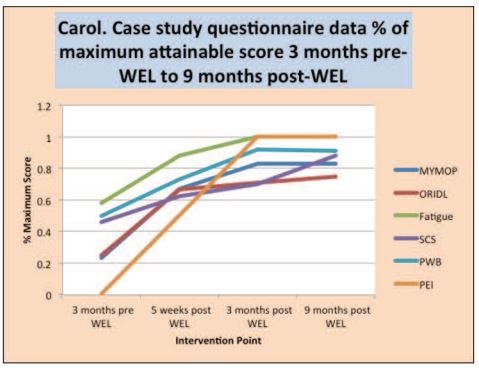
Let’s look at this action. This next example is from a research depth-study of a healing response. The researchers called this woman Carol. She was a healthcare staff member in her early 50s who joined our wellness enhancing learning programme in the Highlands after 36 years of absolute misery and suffering. The programme (TheWEL) was designed to model what had been learned from the one-to-one studies of supporting healing responses into a group situation.
Carol’s pre-three-month interview:
- Depression every year for the last 36 years, as troughs in an overall pretty miserable existence.
- Anti-depressants on a seasonal basis.
- Periods – unable to leave the house for nine months.
- Anxious all the time, ‘fear’ is a central theme in her life.
- Panic attacks ➟ urinary incontinence and vomiting.
- Paranoia and self-loathing also feature.
- Not many people know her suffering, she can put on a face.
I know that had I met this person before the mid-1980s I would have had a very heart-sinking feeling. Now, I know she has transformative potential, not through faith, but because of simple, practical experience. I know the seed may be buried in the permafrost under ten feet of concrete, and I know this may be a five-year job, and a very stormy job at that. But I know she can shift. When she came back three months after entering the programme, the PhD researcher who re-interviewed her noted ‘an absolute shift in her manner… a deep transformation… a changed awareness and ways of being with herself’.
Carol – interviewed after the course
+3 months: Carol described how every dimension of her life had changed and she was off all drugs. In her own words,
‘[It’s] Totally different.The whole way I look and see things and feel things… I keep pinching myself that I’m not dreaming all this… I’m not afraid anymore… this confidence is coming from inside it’s not just a phase… I’m myself now, I’m quite happy with who I am.’
I’m healing, I see myself as healing.This is just a personal thing, I’ve seen myself with like an open wound that’s never healing, and now I can see it’s closing down you know it’s like you know how if you’ve got a scar it’s open, so now this is closing in, its healing, that’s how I feel. It’s not open anymore’.
+12 months:
I have to say this, this is the first year, since I was 20, that I never had to take anti-depressants or St John’s Wort or something like that for my mood swings, because I have suffered from depression all my adult life’.
When the shift happens and the seed germinates the effects ring through the whole organism: different dimensions that practitioners didn’t even know about begin to reorganise. I’m still amazed by this – by my old maps it’s not supposed to happen, especially after so many years, nor so quickly. This doesn’t happen all the time of course, but as an explorer, once I had seen it, I now knew it could happen. It was experiences like this that led me to more formal study and research. The research team’s results show that Carol’s results echo the group averages, as does a series of in-depth case studies and qualitative work. Our main research work also used the six measures shown in Carol’s results in Figure 4, tracked prospectively with some randomised wait list groups. The results showed clinically important and statistically significant improvements in all six measures, across the whole time period. This confirmed the years of course assessments, and the pilot research results (Higgin et al, 2009), and the retrospective tracking. The same was true of our quantitive measures. Fasting insulin levels are a sensitive measure of movement towards diabetic risk, and in our study cohort of 125 people just less than half were actual or suspected pre-diabetics. After the course, half of those with raised insulins had improved, and one in three of those in a ‘pre-diabetic’ category moved out of category, persisting at nine months. (Reilly, 2013a, Reilly et al, 2013a; Reilly et al, 2013b).
What are we dealing with here? Rich questions arise. How can we now learn better to catalyse such germination, engage it and foster it effectively? How can we best measure its effects? What might its determining conditions be? What are its limits? Can it be taught? Can it be scaled up?
 There is clearly more going on than the important elements of inspiration or motivation or willpower. One core dimension is a deep shift in perception, with a resultant reconnection to capacities. In time, this entails a physical shift in the embedded patterns of mind. The subconscious maps or mindsets we navigate our lives by become physical: the more you think a thought or hold a view or map your world a certain way, the more the brain myelinates these pathways and insulates them. These are the sorts of map that drive your car when you’re not thinking about it. And they drive your inner and outer life. When you shift the map, the journey changes automatically, it has to. Then what about our own maps?
There is clearly more going on than the important elements of inspiration or motivation or willpower. One core dimension is a deep shift in perception, with a resultant reconnection to capacities. In time, this entails a physical shift in the embedded patterns of mind. The subconscious maps or mindsets we navigate our lives by become physical: the more you think a thought or hold a view or map your world a certain way, the more the brain myelinates these pathways and insulates them. These are the sorts of map that drive your car when you’re not thinking about it. And they drive your inner and outer life. When you shift the map, the journey changes automatically, it has to. Then what about our own maps?
The practitioner shift
Our colleagues are dropping on the battlefield, burning out in increasing numbers. As the relevance of self-care and self-compassion for health practitioners became clearer to me, in 2010 I stared running the original patient groups just for the staff – The StaffWEL. The staff often seemed as unwell as their patients or clients. Why is that? Are we saying, ‘Okay plant, I won’t be watering you because I’ve got everyone else’s plants to water’? Whatever the mixed causes, we need to confront this neglect: would you treat a dog the way you treat yourself? I’d bet you wouldn’t dehydrate it, feed it the junk you feed yourself, or the alcohol, or subject it to the self-attacking voice in your head, or the stress you put yourself through, or starve it of exercise or activity, or play, or downtime or calmness or sleep. Go find these maps – mostly now subconscious – that drive this life-neglecting way of living. Then enter the journey to shift them.
Life-compassion
What works is an activation of a self-sustaining transformation of self-care. In turn, a key here is nurturing-instinct – a given wisdom in us all. In turn, this is automatically mobilised by compassion – another given, but often neglected, capacity. In our staff and patient groups we found measures of self-compassion rose significantly over the nine months. But the self we are talking about here isn’t the egoic self. More accurately the shift we aimed for, and the one people described, was in compassion towards their life, rather than ‘self’ compassion – and this life-compassion cascades nurture with its intrinsic respect for life. Not that people would necessarily articulate things this way – indeed they often struggled to find words to describe the shift, even saying ‘I don’t know what happened, but things have changed’.
The vision of this plant, instead of someone saying, right, you’ve got to look after yourself, we all know that. The visual element of the plant sitting…I thought… oh my God, my roots are all dry. I’m not grounded and my petals are all faded. But gosh, that really worked for me.
WEL patient participant, 2012
We experience the world as we see it. We can see your life-predicament, our darkness, in flight or fight mode, as an enemy and we shrink or attack accordingly; or, we can see it as a plant with drooping leaves crying out for the nourishment only the keeper of that life can bring. This transformation of our perception of suffering involves a shift towards a felt sense of a larger, truer, deeper self: a realisation that I am not the waves, I am the ocean. Call that what you will, but watch out for the web of labels.
When a human being experiences that movement, something very profound happens, and we have seen how directly accessible that shift can be when circumstances are right, triggering transformative process. Wisdom traditions, spiritual and religious teachings have emphasised this, but all too often they distort the story so that the shift seems distant, externally mediated, unattainable. But I believe it’s actually robust, ever-present and natural. It is after all only a reconnecting to what we might call the wellspring: the pre-existing and fundamental characteristics of life itself – repair, growth and flourishing – with the natural fruits of joy, peace, creativity, spontaneity, loving, openness, connectivity. Yet when we speak of such things, and even though these traditions have a thousand ways of talking about them, we actually enter a territory where language fails. Perhaps the great task of our time is to reclaim this realm in a secular context, and so retrieve the wisdom that lives in all of us and rediscover these instinctively available and naturally inherent capacities.
The fifth wave
The idea and metaphor of a needed fifth wave to meet the new public health challenges was seeded by the Public Health Institute of Scotland headed by Professor of Public Health Phil Hanlon. Andrew Lyon led country-wide learning journeys of an enquiry group seeking inspiration. They concluded that the capacities that Carol modelled contained the essence of a new way (Hanlon et al, 2011a).
How can we take what we’ve just seen and scale it to a level of a nation?’ This was the bold visionary question that Phil Hanlon asked me in 1999 after meeting one of my patients who had shown a healing response similar to Carol’s. This wonderful question is akin in scale to the dream of Loch Katrine’s water supply. You know, the rock they had to get through to create those 19th century tunnels was so hard at times they advanced only a meter in a month. Phil’s question was part of my inspiration to ask if we could inch-advance into the solution of the epidemics by testing if the effects of this wellness-enhancement-learning approach evident in one-to-one work could be catalysed in a group setting – and so TheWEL was born in 2004. More than 3,000 patients and staff have completed this – and the research has said yes, this can work well in both primary care and secondary care. Now, TheWEL Charity with a sister charity Community Renewal will pilot a facilitated version in community settings. In the big scheme of things this is just a trickle of clear water but it shows the potential for profound personal transformation is there waiting to be mined. Government-backed initiatives have picked up some of the themes of the enquiry – compassion was placed in the NHS quality strategy (The Scottish Government, 2010), and the birth of the ALLIANCE organisation seeded an emphasising on the power of people with long-term conditions to change the course of their own lives (Douglas-Scott et al, 2008). The risk here is of these second horizon initiatives being absorbed into the old ways of our first horizon. Increasing the flow and impact of these fifth wave ways and changes could take a long time to affect the epidemics, but the direction we can travel is clear. Coupling traditional forms of actions to clean up the air and food and environmental toxicity, combined with fifth wave orientation and action over the next 20 or 30 years could bring these epidemics to a halt. If it can become an embedded norm to ask what they can do to help release innate capacity and healing, this can spiral out from the individual to touch families, communities and nations.
What if the whole medical toolkit became servant not master of this vision? Imagine what would happen if we placed the capacity for innate healing movement and change, of repair and growth, and so flourishing at the centre of our vision and so into the design of our services and our science? Transformative change would grow as people like Carol lead us out of this dark era.
Acknowledgements
To Carol and my thousand other teachers, to all my colleagues on the Healing Shift Enquiry and WEL programmes – too numerous to list – but some mentioned below as authors in the references.
- thehealingshift.org; www.thewel.org; www.afternow.co.uk BBC (2014) The rise of Glasgow urban growth in Victorian Scotland (cholera epidemics). Available at: bbc.co.uk/history/scottishhistory/ victorian/features_victorian_urban.shtml (accessed 12 March 2018).
- Campbell J (2008) The hero with a thousand faces. The Collected Works of Joseph Campbell. Ovato, CA: New World Library.
- co.uk (2015) Five Scottish children diagnosed with type 2 diabetes. Available at: www.diabetes.co.uk/news/ 2015/jan/five-scottish-children-diagnosed-with-type-2-diabetes-97211814.html (accessed 12 March 2018).
- Douglas-Scott S, Donaldson A (2008) Gaun yersel: the self management strategy for long term conditions in Scotland. Edinburgh: The Scottish Government. Available at: www.alliance-scotland.org.uk/ blog/resources/gaun-yersel/ (accessed 12 March 2018).
- Hanlon P, Carlisle S, Hannah M, Lyon A, Reilly D (2012) A perspective on the future public health practitioner. Perspect Public Health 132(5): 235–239.
- Hanlon P, Carlisle S, Hannah M, Reilly D, Lyon A (2011a) Making the case for a ‘fifth wave’ in public health. Public Health 125(1): 30–36
- Hanlon P, Carlisle S, Hannah M, Lyon A, Reilly D (2011b) Learning our way into the future public health: a proposition. Journal of Public Health 33(3): 335–342.
- Harcombe Z (2010) The obesity epidemic: What caused it? How can we stop it? York: Columbus Publishing.
- Higgin M, Reilly D, Mercer S, Hopkins D (2009) Evaluation report of the pilot phases of the wellness enhancement learning programme for patients with chronic fatigue syndrome CFS-ME. Available at: www.thewel.org results (accessed 12 March 2018)
- McCombes A (2010) Loch Katrine; a triumph of community values over private greed. The 150th anniversary of the greatest public health achievement of its day. Available at: http://eastdunbartonshiressp. blogspot.co.uk/2010/01/loch-katrine-triumph-of-community.html (accessed 12 March 2018).
- Reilly D (2013a) The healing shift enquiry – creating a shift in healthcare. Journal of holistic healthcare 10(1): 9–14.
- Reilly D (2013b) We need a new vision to meet the new challenges of our times. Journal of holistic healthcare 10(1): 4.
- Reilly D, Banks A, Clark C, Krawczyk C, Lyon A, Quinn P, Smith F (2013a) Water from TheWEL: The healing shift enquiry – seeding a shift towards a health culture in an ill(ness) environment. Initial Learning from a StaffWEL – Wellness Enhancement Learning – programme. Paper presented at the The Scottish School of Primary Care 2013 Annual Conference, Inverness. Available at: www.sspc.ac.uk/images/PDFs/large/DReilly.pdf (accessed 12 March 2018).
- Reilly D, Banks A, Clark C, Krawczyk C, Lyon A, Quinn P, Smith F (2013b) The Healing Shift Enquiry: creating a shift in health care. Annual Report.
- Reilly D (2001) Enhancing human healing. BMJ 322(7279): 120–121.
- Russ TC, Stamatakis E, Hamer M, Starr JM, Kivimäki M, Batty GD (2012) Association between psychological distress and mortality: individual participant pooled analysis of 10 prospective cohort studies. BMJ 345: e4933.
- Sharpe B (2013) Three horizons: the patterning of hope. Charmouth: Triarchy Press.
- Sweeting H, Young R, West P (2009) GHQ increases among Scottish 15-year-olds 1987–2006. Soc Psychiatry Psychiatr Epidemiol 44(7): 579–586.
- The Scottish Government (2010) The Healthcare Quality Strategy for NHS Scotland. NHS Scotland Quality Strategy – putting people at the heart of our NHS. Edinburgh: The Scottish Government.
- Visintainer MA, Volpicelli JR, Seligman ME (1982) Tumor rejection in rats after inescapable or escapable shock. Science 216(4544): 437–439.
- Yashina S, Gubin S, Maksimovich S, Yashina A, Gakhova E, Gilichinsky D (2012) Regeneration of whole fertile plants from 30,000-y-old fruit tissue buried in Siberian permafrost. Proc Natl Acad Sci USA, 109(10): 4008–4013.






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}