

Clinical leadership
Daghni Rajasingam, Head of Service for Obstetrics; Deputy Director for Post-Graduate Medical Education, Guys & St Thomas’ NHS Foundation Trust
Published in JHH13.3 – Saving the NHS
I am a consultant obstetrician in a large, urban tertiary hospital serving a diverse local population. I believe in social justice and advocating women’s rights through practising and disseminating women’s health rights both in the UK and globally. I have an academic interest in leadership development and passionately believe that we need to build the resilience of the NHS workforce through understanding systems change and a hosting style of leadership
[bctt tweet=”The NHS workforce are trying to make real a vision of a vital, universal healthcare system” username=”BritishHolistic”]
The NHS Constitution
The NHS belongs to the people. It is there to improve our health and wellbeing, supporting us to keep mentally and physically well, to get better when we are ill and, when we cannot fully recover, to stay as well as we can to the end of our lives. It works at the limits of science – bringing the highest levels of human knowledge and skill to save lives and improve health. It touches our lives at times of basic human need, when care and compassion are what matter most.
The modern NHS’
Within the last decade the NHS has prioritised the importance of safe care, together with high-quality service provision that improves the experience of patients. However, changing demographics of the population and constrained resources, both financial and human, means that services will need to be designed and delivered in radically different ways across traditional boundaries of care. The culture and environment to facilitate this will require a significant shift in ideology from one where the professional is the expert and the patient the recipient of this expertise, to one where there is a more equal partnership-based relationship, where providers, both from the acute and primary care sector, users and stake[1]holders share responsibility and work together to find sustainable solutions.
Our NHS landscape has been deluged by a tsunami of reforms over the last 10 years, culminating in the Health and Social Care Act 2012, an unprecedented period of healthcare institutional failings (Mid-Staffordshire Hospital , Morecombe Bay Hospital and the Keogh 14) and a shrinking financial purse. With ‘clinical leadership’ emblazoned on every single signpost, we have had to reconsider what we mean by leader[1]ship and to challenge some of the traditional notions of leadership. Much of the published healthcare leadership discourse focuses on managerial concepts, meanings and framing of the term ‘clinical engagement in leadership’. The assumed passivity of the clinician is a common thread. And yet, most clinicians have the closest relationships with patients and are potentially the ones with the most influence and moral obligation to do their best.
An outsider’s perspective
In 2013, Don Berwick was asked to review the NHS in the light of the Mid-Staffordshire Francis report (Francis 2013). Berwick, in his letter to clinicians, managers and all the staff of the NHS, talks of being impressed with the NHS workforce of ‘1.3 million people who are trying to make real a vision of a vital, universal healthcare system, accessible to all and free at the point of service’. In addition he was impressed with the UK’s commitment to healthcare as a human right and to healing as a shared social mission. Despite being clear in his letter that some standards should be rigorously enforced, he also acknowledged that real, sustainable and active improve[1]ment depends far more on learning and growth than on rules and regulations. He says that in an ‘all teach-all learn’ culture, ‘measurement is not a threat, it is a resource; ambition is not stressful, it is exciting; defects are seen as opportunities to learn; and curiosity abounds’.
The four guiding principles he recommends are:
- placing the quality and safety of patient care above all other aims for the NHS
- engaging, empowering and hearing patients and carers throughout the entire system
- fostering wholeheartedly the growth and development of all staff, especially with regard to their ability and opportunity to improve the processes within which they work
- insisting on, and modeling in your own work, thorough and unequivocal transparency, in the service of accountability, trust and the growth of knowledge.
A clear understanding of ‘quality’ and systems thinking, co-production, quality improvement methodology and reflective team practice seem to be the bedrock of a sustainable, learning healthcare system.
Patients are the most under-used asset in the NHS
For some time now, it has been recognised that patients are the most under-used asset within the NHS. In areas where their experience and expertise have been harnessed, service provision has been transformed with reduction in demand for clinician input. Traditional pathways and inappropriate skill mix are barriers to thinking innovatively about designing radically different ways of providing high-quality care. Co-production means delivering public services in an equal and reciprocal relationship between professionals, people who use
Patients are the most under-used asset within the NHS
services, their families and their neighbours. Where activities are co-produced in this way, both services and neighbourhoods become far more effective agents of change. By involving people in the delivery of their own services, co-production shifts the balance of power, responsibility and resources away from professionals and into the hands of individuals and communities. It recognises that ‘people are not merely repositories of need or recipients of services’, but the very resource that can turn public services around. Co-production also means unleashing a wave of innovation wherever services are designed and delivered. Though the NHS has tried to institutionalise co-production, in its essence co-production has to bring the actions of individuals in communities together with the people who have the authority to make decisions. Consequently this process of doing with, rather than doing to, or doing for, calls for a fundamental shift in power away from top-down hierarchy and into partner[1]ships based on network relationships.
Clinical leadership styles
Clinicians need to take ownership of the current challenges their services face. They have to demonstrate leadership by influencing their provision at all levels – from the frontline to the political sphere. How they choose to lead, though, may determine their success or failure. In the context of the NHS two different kind of leadership are needed. Transactional leaders focus on the task and targets and manage performance. They focus on the practicalities of the job and turn ideas into reality. The transformational leader, however, changes the way that people think about themselves, by focusing on new possibilities, and turning visions into ideas. Within the complex political framework of healthcare provision in the UK, coping with increasing numbers of policy and legislative documents relating to commissioning and provision of services, has given transactional management and leadership an important role. However, senior management is pulled in two directions: on the one hand they want us to practice in novel ways in order to make cost savings, but at the same time we are expected to improve the patient journey. But, understandably, given the structural turbulence of legislation, a certain kind of inward focusing has made the necessary new relationships with other organisations – which would be required in order to do more and better with fewer resources – even more difficult to build. Even though transformational leadership rhetoric is ever present in NHS leadership frameworks, the realities of structural and financial restraints generally stifle it. Nonetheless I believe that if we can develop a style of leadership based on ‘hosting’ we might realise the powerful and positive asset base which our patient populations and NHS staff represent and, that this could potentially overcome the undeniable structural restraints we face.
Why clinical leadership
There is evidence to suggest a strong link between medical leadership and organisational performance. For example, when the introduction of total quality management into the NHS was evaluated, there was an intricate link between how well it was applied and how engaged doctors were. McNulty and Ferlie (2002) echo these findings in their report on business process re-engineering in Leicester. The US literature found similar results; for instance Watson and Kimberly (1997) emphasised engagement of doctors as one of the key facilitators for successful reconfiguration.
Much of the discussion about engaging doctors in management has been based on a deficit model which assumes there are identifiable managerial skills and areas of knowledge which doctors have not acquired. This over[1]looks the process of management as a social and political process, which many doctors may have an aptitude for and indeed experience of. There is an assumption that doctors must ‘become’ managers, a position which some sceptical colleagues see as an expedient viewpoint constructed by managers. The question rarely posed however is how it might be possible to have organisations that are truly clinically led but with managerial enablement.
Tribalism is strongly ingrained in many healthcare professional groups. Clinicians who occupy ‘hybrid’ roles have a challenging time bridging the gap between two cultures. In addition, the tendency of professional tribes to orientate towards stability rather than change generates a host of problems. To overcome these inherent obstacles to innovation we need to move towards appointing large numbers of doctors to leadership roles while accepting that some of these leaders will not require formal positions in the hierarchy. Instead the emphasis should be on collegial and horizontal control processes. Yet even new forms of leadership alone cannot deliver the transformational change the NHS is desperate to implement, so these new
Clinicians who occupy ‘hybrid’ roles have a challenging time bridging the gap between two cultures
forms of medical leadership need to be developed along[1]side other strategies. Most importantly these leaders need to be nurtured, supported and valued by strategic leaders at all levels of the NHS.
Can transformational leadership be encouraged, developed and sustained? The complex external forces now operating on clinicians are seldom understood. Leadership, though it must come from within, also requires strategic nurturing early on in clinical careers and especially so during transitional periods between jobs. In order to make this a reality, a non-negotiable assessment of self-awareness, reflective practice, commitment to quality improvement and resilience should be integrated into would-be medical leaders’ appraisal and revalidation processes. The standards already proposed by the Faculty of Medical Leadership and Management would go some way towards ensuring this.
Models of clinical leadership
Having examined several different frameworks around clinical leadership, I have found none that fully reflect the complexity of leading individuals and teams that provide patient-focused, quality care within the today’s turbulent environment of financial and time constraints. In most existing models deeper clinical perspectives are lacking. Based on my own action research into ‘what makes clinicians tick’ I have produced a modification of Senge’s systems-thinking framework with the aim of encouraging clinicians to understand systems thinking in the wider context of the NHS. To be effective as individual leaders and members of teams they have to grasp how they fit into this volatile landscape.
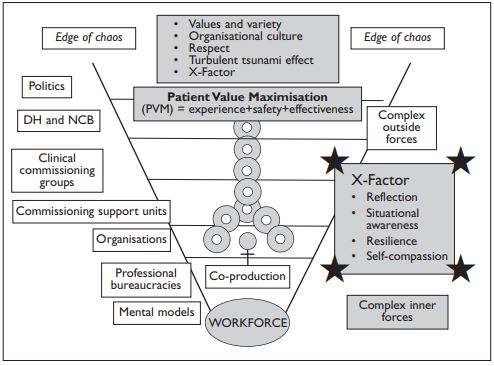
My model incorporates maximal external forces and turbulence at the top of the ‘vortex’ with patients in the centre (the eye of the storm) and staff in close proximity at the base of the vortex, exerting complex inner forces (mental models and professional bureaucracies) and providing a relatively stable foundation for the vortex. A service delivery chain extends from the chaotic political environment at the top through regional commissioning groups to provider organisations and ultimately as far as the patient. If the sole aim is to maximise value for patients (patient value – PVM) then striving for a stable and unchanging environment is likely to be unsuccessful. Instead we will need to be self-aware, adaptable and flexible in order to thrive in the present climate and ‘save the NHS’.
Fundamentals of resilient organisations, patients and staff
The ability of clinicians to best exert their ‘X-Factor’, enabling a coupling of external and internal forces, will depend on three factors: their resilience, their ability to reflect and their understanding of systems. Organisational resilience is defined by the British Standards Agency as ‘the ability of an organisation to anticipate, prepare for, and respond and adapt to incremental change and sudden disruptions in order to survive and prosper’. As individuals increase their self-awareness and resilience, the organisation will reflect this. Our healthcare system requires us as professionals, to act compassionately, but until we as a profession give self-compassion the credit it is due, and NHS organisations nurture and respect this quality, what is being demanded of our workforce will be neither fair nor deliverable. Only when we, as parts of the system, understand the crucial role of resilience, reflection and self-compassion as crucial moderators and mediators in the system, will we have it in our gift to ensure that our amazing healthcare system, the NHS, survives another generation.
References
- Francis R (2013) Report of the Mid Staffordshire NHS Foundation Trust Public Inquiry. London: TSO.
- McNulty T, Ferlie E (2002) Re-engineering health care: the complexities of organisational transformation. Oxford: Oxford University Press.
- Watson S, Kimberley J (1997) Re-engineering hospitals: evidence from the field. Hospital and Health Services Administration 42(2) pp 143–163.






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}