

…and breathe!
A key innate resource, hiding in plain sight
A key innate resource, hiding in plain sight
Andrew Morrice, GP; psychotherapist; educator
Published in JHH 18.2-Frontiers of self-care
Breathing – it’s hardly new is it?
Humans, like some other mammals that have since ventured back into the water, can voluntarily control their breathing, overriding the autonomic drives that would otherwise govern every breath. This is almost certainly something to do with the way we evolved our ability to sing and then to speak (MacLarnon and Hewitt, 1999). In parallel we have also evolved the capacity for intense imagination and abstract thought and through them created complex societies and novel physical environments. They in their turn have become unprecedented sources of unrelenting biological stress.
The saving grace, having strayed so far from our wild evolutionary origins, is that by evolutionary accident we’ve been gifted this innate capacity to breathe as if we were already relaxed. When we do this, it alters vagus nerve signalling to the brain, and diminishes the stress-response with its many impacts on our brain and body. Only then can we access our embodied calm, wise, knowing, reasoning and reflecting self. This can restore the capacity for refreshing sleep and reverse many of the unhelpful bodily and biochemical changes that threat-defence reactions provoke. This insight, so ever-present in ancient and spiritual practices, we can now explain in physiological terms. Neurophysiology fully affirms vedic wisdom’s insight that the breath can bring us back into balance (see Streeter et al, 2012 or numerous other papers authored by Chris Streeter or Julian Thayer).
‘Two things are easiest to do. One, to carry water in a sieve. Two, to still the mind. Freeze water. Breathe calm. Only two secrets to learn.’
Swami Veda Bharata
This breath-induced relaxation is thought to be due to changes in parasympathetic ‘tone’ (activity in the vagus nerve) which rebalance the autonomic nervous systems. There isn’t space here to explore the many links between our ‘threat-defence’ responses, including hyperventilation, and ill-health. After teaching this in detail for more than 10 years for doctors and medical students, I have come to a straightforward summary: chronic threat-defence (stress) responses amplify the processes underlying most chronic diseases including ‘functional syndromes’ and many mental health problems. It follows that shifting down and out of these physiological patterns will help in most problematic situations. I am going to describe this mainly in ‘we’ and ‘us’ terms, but all of this can be applied not only for supporting patients, but also in our own self-care and will therefore build our capacity to practice and thrive.
Out of many we are one?
For many years as a clinician with a scientific interest in breathwork I had to grapple with a fragmented and confusing literature, lacking in agreed terminology. Yet many papers said remarkably little about the techniques under discussion (see Zaccaro et al, 2018). Fortunately a recently published review provides a neat summary of our current understandings of breath and the relaxation response. Gerritsen and Bands’ review (Gerritsen and Band, 2018) clarifies that the four fundamental factors present in almost all breathing patterns used in ‘contemplative practices’ all cause changes in parasympathetic activity, evoking a ‘relaxation response’ (a term first coined by Herbert Benson, to be contrasted with the ‘stress response’) (Benson et al, 1974). The relaxation response in turn supports attentional shifts, which in day-to-day life improve access to memory, thinking and reflection skills. Other lines of research highlight increases in alpha-wave brain activity brought about by these breathing patterns.
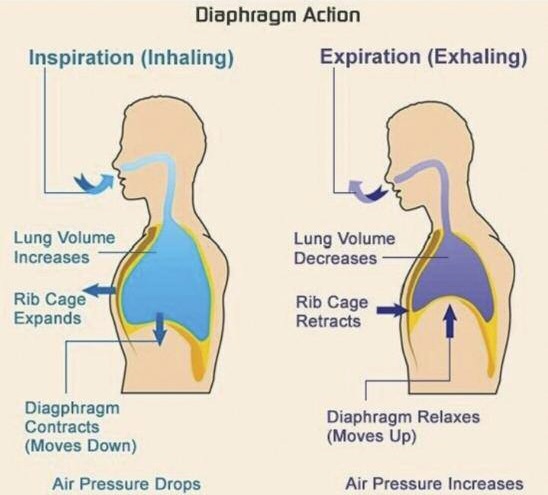
The effective breathing pattern is close to six cycles a minute (in adults), in which inspiration occupies less than half the breath cycle. Most of the air movement is produced by the diaphragm with minimal activity in the muscles of the chest and abdominal walls and is allowed to happen without being controlled or forced. Notice that breathing through the nose (often emphasised in yoga) is absent from this list. Nasal breathing is our default pattern and usually helpful, but as there are so many other physiological mechanisms at play, we need not insist on it.
Out of one, many!
These fundamental features are present in remarkably diverse practices, not just the ‘contemplative practices’ covered by the above review. In my clinical experience, understanding the commonalities and differences between them has given me a better chance of connecting patients with their innate relaxation response. If a person has previously been taught about breath in another context, knowing of their prior experience will help us agree on further options and build on any relevant skills or move past any difficulties they might have encountered. In making sense of the diverse options, we need to understand the main differences, as well as what they all share.
The most obvious one is the counting pace used in the practice. Some systems use a pace of approximately one beat per second (for example in 4:6 – inspiration 4 counts, expiration 6). Others use a faster counting pace of about 100 beats a minute – about the fastest pace numbers can be comfortably counted aloud. This gives an inspiration-expiration counts of around 7:11.
A second variant is whether a pause or hold is explicitly built in at the end of the in-breath, and whether a second pause is included after the out-breath: for example an inspiration-hold-expiration count like 4:7:8 or 4:2:4 ‘box’ breathing. Other techniques, notably Buteyko, use a long pause at the end of the out-breath.
A third and much larger source of variation is the complexity and extent of further elements to the practice. For example HeartMath training combined a number of elements (breath pace, breath focus and emotional state recall) into a single instruction. CardiacCoherence (which is similarly concerned with heartrate variability) tends to focus first of all on pace. Buteyko programmes too teach more than breathing techniques. Yoga and Taijiquan both combine significant elements of movement and different poses, and, if taught traditionally, a rich corpus of embodied attention techniques. They also entail breathing patterns that differ significantly from those described above.
A fourth source of difference and potential confusion is brand-related language. For example some mindfulness scripts are indistinguishable from hypnotherapy trance-induction and relaxation scripts, in that all use attention shifts, breath cueing and re-pacing. So while featuring in hypnotic induction, the same basic breath cycle might be described as ‘relaxation’ ‘mindful’ or ‘coherent’. This language issue is particularly striking with regard to the many hundreds of apps that incorporate breath pacing.
A fifth dimension is the extent to which attention is managed in combination with the breathing pattern: in many meditation techniques attention may be directed in many ways, or none. As already mentioned many audios, apps and therapeutic tools are designed to alter attention.
Lastly the significant breathing pattern may be embedded but not spoken about in apparently unrelated activities. Examples include playing wind instruments, singing, chanting and some styles of smoking and vaping.
Allowing or pacing?
We also need to be alive to the polarity between, at one end of the scale, a classic mindfulness approach within which breath, along with the content of the mind, is simply observed, and at the other end, a clear instruction to follow a pre-determined pattern of breathing. Clinical and personal experience suggests that the latter is particularly helpful where a person needs distraction from profoundly troubling cognitions and/or is in a very heightened state of arousal. Yet sometimes this more deliberate style can feel forced, and there is a chance of worsening hyperventilation unless tidal volume is kept low (instruct for ‘deep breaths, not big breaths’). But in lower states of arousal, already reasonably close to the relaxed/relaxing pattern, or for performance anxiety or perfectionism, purely allowing the breath to do what it is doing can be most helpful. This is also best suited for developing the other skills taught in mindfulness practices.
For many people the ideal lies somewhere between; the ‘allowing’ mode may call for some prior learning and practice of a calming pattern. Once familiar with what it feels like when the body relaxes and mental chatter dies down, we can slip with increasing ease into the more spontaneous ‘allowing mode’ of slow unforced breathing.
Some relevant science
A number of physiological mechanisms have been proposed to explain the benefits of better breathing: improved parasympathetic activity and less volatile sympathetic drive, along with more rhythmic interplay of parasympathetic and sympathetic drives; increases in alpha-wave activity (alpha waves in the electroencephalogram (EEG) indicate a normal wakeful state of quiet rest); and getting dissolved blood gases (oxygen and carbon dioxide) back into their resting balance. Many of these form positive feedback loops and they can be assumed to be working synergistically.
The breath practices described boost ‘vagal tone’. This increased signaling from the body to the brainstem via the vagus nerve synchronises with the normal six cycles a minute rhythmic rise and fall of blood pressure and amplifies it. (For more details on the arterial baroreceptor reflex see Julien, 2006). In addition there is increased signalling to the brain stem from pulmonary stretch receptors in the lungs and from receptors within the nasal vault via olfactory nerves, to the frontal cortex which in turn tunes its attention-directing activity.
So far, so physiological. But there are whole body and mind effects too. The body-mind ‘interocepts’ our ‘internal ‘environment’: that is to say we unconsciously ‘notice’ messages from the body. We learn to recognise these patterns, very often as emotions. So for instance ‘interoception’ of rapid breathing patterns are very likely to be registered as alarming. Slow diaphragmatic breathing on the other hand, even if brought about voluntarily, usually signals safety, calm or wellbeing. This allows further de-arousal and relaxation either subconsciously or consciously. In tandem, this redirected embodied attention diverts the mind away from unhelpful self-talk, rumination or catastrophisation. This helps calm the anxious mind’s ‘top-down’ reinforcement of the anxious body’s threat defence (stress) responses.
A number of physiological mechanisms have been proposed to explain the benefits of better breathing
Your granny was right…
Several practices (including the age-old advice to ‘take a deep breath and count to ten’) accentuate the pulmonary stretch receptor effect. These include ‘box breathing’ (4:2:4) and the particular pranayama technique rebranded by Andy Weill (4:7:8). Simultaneously these practices also help re-establish normal levels of CO2 dissolved in the blood. When CO2 is lowered by hyperventilation a cascade of chemical changes reduce blood calcium to levels that alter sensation, muscle function and cerebral blood flow.
A drawback of granny’s advice is that people often confuse ‘deep breathing’ with chest expansion. In fact the opposite is the case. Yet I find that diaphragmatic breathing is easier to re-establish for some than others. In my experience with patients who can’t rapidly access the diaphragmatic breathing pattern I have learned it is best to leave this aside and focus initially on pace and reducing tidal volume. It is helpful to have multiple techniques to hand to re-institute the default diaphragmatic breathing pattern and draw on these once the patient is sufficiently relaxed to engage with them.
These stories about patients illustrate a few points with regard to self-care. The first is that either of them could have been me. We’ve all been there. I certainly have. Once we are caught up in a significant stress response the narrowing of our attention on to threat-defence or responding to demanding circumstances means that we may for the time being either forget, or simply not feel it is appropriate to relax. Such stories also help patients understand not just how transformative the slow deep breath-work can be, but also how easy it might be not to notice, and not to practise, and not to build it into our lives.
How easy it can be to underestimate the power of something so apparently trivial and simple as breathwork. Most modes of relaxation – social engagement, absorbing activities, play, exercise, and green spaces – involve a time and a place, logistics and circumstances. Yet the relaxation response engendered by slow diaphragmatic breathing is both a very internal and a completely innate resource. For the breath is always with us, and we can change it to find our way to calm ‘any time, any place, anywhere’ (like Martini, if you are old enough to remember those ads).
‘But it didn’t work for me doctor’
We may hear this surprisingly often when we start to talk about using the breath. For many of my patients, ‘breathing’ has joined their long list of things that ‘didn’t work for me’. It is almost always the case that they learned about it without enough support and attention to ensure it was actually working well enough to help. Two to three minutes of slow diaphragmatic breathing will calm you beautifully if you are mildly stressed and your amygdala isn’t carrying the imprint of multiple traumas. If you are close to panic or profoundly conditioned to respond to the world as threatening, it just won’t do the trick. You’re likely to need about the same length of time it takes a diazepam to activate the self-same GABAergic brain centres: 20 minutes or so.
And there are other obstacles. For instance embodied trauma can manifest as ingrained tension and constrictions in abdominal, chest and shoulder muscles. Letting go of these defensive postures and finding confidence to let down the guard around the belly may call for physical and psychological therapies. These things need insight, time and skillful support.
It may be that our associations with the context we learned about the calming breath aren’t positive. ‘My yoga teacher raped me’ was one patient’s barrier. Or that we felt the practitioner wasn’t quite getting us or our problems, when they briefly touched on box breathing – that it seemed completely disconnected from our problems and suffering at the time.
Creating a meaningful ‘bridge’ between the very wide range of difficulties in which vagal respiratory stimulation can help (anxiety, depression, anger, addiction, pain, unrefreshing sleep, fatigue, burnout, symptoms typical of hyperventilation), and the technique itself is crucial. This usually involves ‘working with’ or extending the patient’s current model of reality. Without a connecting map and believable context, whether of mind–body connectedness or nuts and bolts body-function, the idea that better breathing could be a solution to a chronic predicament just isn’t going to be credible.
Having understood the why, the how can follow once a person is prepared to change. Even for (especially for?) someone who desperately needs self-regulation skills, regular practise may seem impossible. Setting aside enough time for practise, makes a vast difference, but for anyone who is poor at forming routines, too distractible and or busy, remembering to engage in breath-work as a regular practice will be a challenge. Yet without it they won’t access this powerful tool in the stressful situations when it’s most needed.
Practise, practise
We tend to stick with things we enjoy. We might stick with things that help, but put them aside once we feel ‘fixed’, or when they just aren’t fun enough anymore. The way I have integrated breathwork into my own life may be relevant, and illustrative. In Taijiquan and Qigong there is a particular sequence of moves that take just 15 minutes. In the morning this engages my otherwise jiggedy mind and brings me completely into my breath and body. At night 10 to 15 minutes of Qigong and Dao Yin exercises before bed sets me up for a better night’s sleep. That’s what works best for me. But for someone else it could be singing, chanting, regular mindfulness practice, counting the breath, yoga, an app or an audio method labelling itself as coherent, mindful, meditative, relaxing or any mix of these.
Whatever your way, practise, practise, then, because ultimately nobody else can do this for you. We all have to find our way in, but we also have a duty of care is to help one another find the doorway that works best. We need each other, not just to learn how to use our breath, but to be there to keep reminding ourselves of this apparently very simple thing. We can’t always self-care on our own. Self-care is a social undertaking.
Andrew Morrice’s current set of resources to support breathwork can be found at www.joineduphealth.net/relax#allresources
- Benson H, Marzetta B, Rosner B & Klemchuk H (1974) Decreased blood-pressure in pharmacologically treated hypertensive patients who regularly elicited the relaxation response. The Lancet, 303, 289–291.
- Gerritsen RJS & Band GPH (2018) Breath of life: The respiratory vagal stimulation model of contemplative activity. Front Hum Neurosci,12.
- Julien C (2006) The enigma of Mayer waves: Facts and models. Cardiovasc Res, 70, 12–21.
- MacLarnon AM & Hewitt GP (1999) The evolution of human speech: the role of enhanced breathing control. Am J Phys Anthropol, 109,
341–363. - Streeter CC, Gerbarg PL, Saper RB, Ciraulo DA & Brown RP (2012) Effects of yoga on the autonomic nervous system, gamma-aminobutyric- acid, and allostasis in epilepsy, depression, and post-traumatic stress disorder. Med. Hypotheses, 78, 571–579.
- Zaccaro A, Piarulli A, Laurino M, Garbella E, Menicucci D, Neri B & Gemignani A (2018) How breath-control can change your life: a systematic review on psycho-physiological correlates of slow breathing. Frontiers in Human Neuroscience, 12.






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}