
Adverse childhood events: what next now we know?
Margaret Hannah, Director of Health Programmes, International Futures Forum
Jacqueline Nugent, Service delivery manager, LinkLiving Ltd
Published in JHH 18.3-Shifting the paradigm
Background
Epidemiological studies since the late 1990s have found links between ACEs (see Box 1) and poorer health outcomes – both in terms of behaviours (eg smoking, alcohol and drug use) and in physical and mental illness (heart disease, cancer, anxiety, depression and suicide). Epidemiologists also report on the high prevalence of ACEs in population surveys and calculate the high population attributable risk associated with ACEs for different conditions. Other studies point to the high economic costs to society and the avoidable burden of distress and disability.
Policy responses
In the early 2000s the Minister for Health and Community Care in Scotland commissioned a short-life working group on responding to survivors of childhood sexual abuse. The group noted a paucity of information about adverse childhood experiences (there is no Read code for example to record this as a reason for attending a GP) and the predominance of service responses aimed at those who had high needs, with far less attention given to the many who went unrecognised in services. It recommended a national strategy to address this, which was launched in 2007 as the Survivor Scotland strategy.
A cross-party working group was established in the Scottish Parliament which maintained momentum on this issue leading, for example, to an independent enquiry into abuse in children’s residential homes. An early adopter of a ‘trauma-informed’ approach was the Violence Reduction Unit, part of Police Scotland, in response to the link between adverse childhood experiences and adult criminality. Interest in this work sparked interest for training and development across other public agencies but an integrated approach to policy and practice is still in its infancy.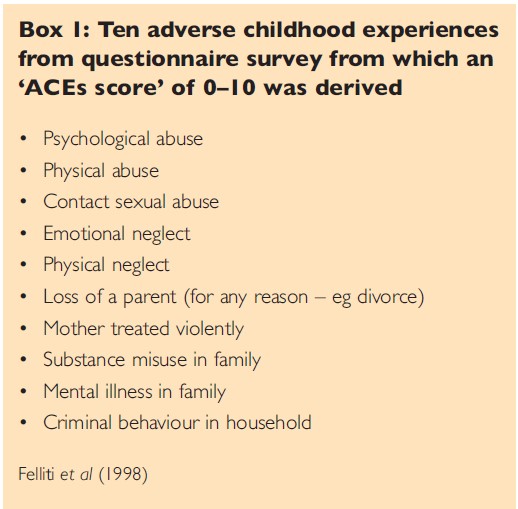
Local responses
Trauma networks involving local professionals working in the field of rape and sexual abuse, domestic violence, mental health, addiction and social work services, public health and health promotion now exist in many areas of the UK. Waiting lists and waiting times for specialist counselling are often long and funding is tight. Demand for services often increases following media coverage of high-profile cases such as Jimmy Saville and more recently the Canadian residential schools.
Practitioners often report the importance of responses that are easily accessed and timely. Clients should be seen within days, not weeks or months. This is a daunting challenge against a background of long waiting lists, but a rapid response aims to provide safety and stabilisation based on an understanding of the effects of abuse rather than to address its content in detail. For many survivors, having better coping strategies can empower them to develop healthier relationships with family, partners and friends, which restore their confidence in moving on in their lives. Others find a psycho-educative approach prepares them for the deeper work they need to do once they are ready to engage with specialist counselling and therapy when they eventually do get seen.
One example from work in Fife
Funding from the Scottish Government Primary Care Modernisation Fund provided the opportunity to try out a responsive, trauma-informed model in primary care, starting at small scale. We called the project Better Than Well on the basis that those who come through adversity can become more active citizens than those who have not had such difficult challenges.
Better than Well is a free service for people aged 16+ who have experienced abuse or neglect in childhood. The service is delivered by Scottish-based charity LinkLiving in partnership with NHS Fife. Eight sessions of cognitive behaviour-based, trauma-informed, self-help coaching are offered to those referred (including self-referral).
The self-help coaches use a range of methods to recognise and manage behaviours and develop coping skills including:
- psychoeducation to help people understand about brain development/potential impact of childhood trauma on children
- working with individuals to recognise triggers and develop an understanding that the reactions to these can be worked on and altered
- assisting individuals to adopt relaxation techniques/ self-soothing skills that are suitable for them.
The service began in 2016 in just two GP practices (a population of roughly 10,000 eligible). Early evaluation from this pilot work suggested the response was welcome from both client and GP perspectives and areas for improvement were identified, particularly in improving access in a timely way.
In 2018, funding from the Survivor Scotland Support and Innovation Fund enabled the project to expand to all residents in the Kirkcaldy and Levenmouth localities of Fife (roughly 120,000 population).
The service became accessible to a range of agencies, not just GPs and clients themselves. The only criteria for a referral were if a person had experienced childhood trauma and they felt ready to work with a coach to look at safety and stabilisation techniques. On receipt of a referral, the coach made contact within two working days and would organise a first appointment within two to three weeks. Appointments were arranged at community venues so clients could attend them in their own area.
In 2019 and 2020 with funding from a mental health fund, the service gradually became Fife-wide (population of 370,000). As part of routine monitoring over this time, data on CORE-10 – a measure of wellbeing – was gathered. 130 clients completed baseline and completion surveys by the start of 2020 which demonstrate a significant improvement in scores between start and end of their eight-week engagement with Better Than Well.
Learning better coping strategies and focusing on personal outcomes for engaging with the self-help coaches has led to many reporting improvements in their lives in qualitative feedback.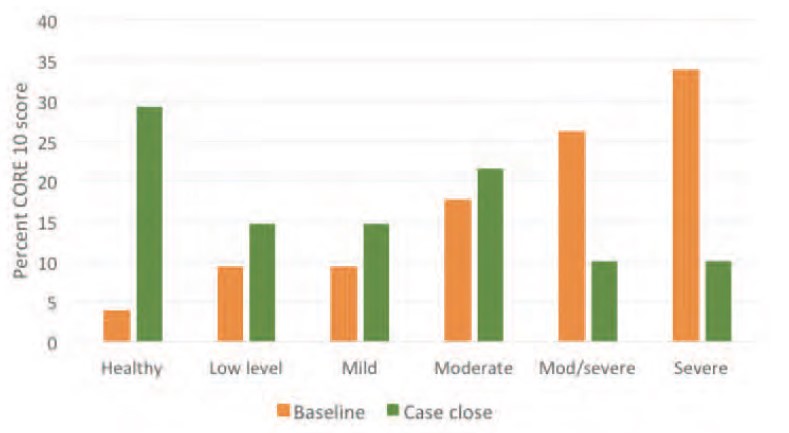
Shared learning events are organised each year to look at progress and discuss how working links between services can be strengthened and widened. This means the service co-evolves with its referring agencies and local links to other sources of support that clients can turn to. For example, staff in other agencies have commented:
‘Sometimes by the time I see clients, after they have been with Better than Well for eight sessions, their baggage is gone and they have nothing hidden to hinder recovery when we come to work with them. That’s a real positive.’
‘If someone needs counselling, they can wait for up to a year to access it through their GP. Our waiting list for counselling is between three and five months. So Better than Well provides an ideal opportunity to bridge this gap, and a solid foundation so that we can address issues more effectively when they come to us.’
‘We use the service on a regular basis. We were looking for a resource for people who were not in need of psychology but who needed support with life skills, and techniques that they could use instead of, or before, going to clinical psychology.’
Some anticipated impacts for NHS services identified through client feedback are:
- reduced demand for NHS services – both community and hospital-based, for example presentations at GP and/or A+E
- reduced prescription costs from reduced need for medication
- clients accessing NHS psychology and other mental health support services may not need as intensive (frequency of use) or extensive support (scale and complexity of use)
- more appropriate targeting and use of NHS services by those who must overcome barriers to access support.
Clients report that their understanding of the impact trauma can have has increased; they take away tools and techniques which they use as the need arises. Coaches also report clients noticing an improvement in their personal relationships.
‘Better than Well has helped us as a family. My girl is happier and so am I. I can spend more time with her without getting stressed out. It’s a happier home here.’
Wider implications
It is important to understand that behavioural health problems (over-eating, smoking, alcohol and drug misuse) may actually be solutions for people who have been psychologically traumatised. People need viable alternative coping strategies and psycho-educational approaches can be highly effective.
For services to become trauma-informed, they need to assume a history of ACEs in all patients and staff – nearly half of the general population are likely to have been affected in one way or another.* We need to be curious about behaviours, listen and be patient with people. Blame and shame needs to be replaced with understanding and patience: we can and do recover from dysfunctional patterns of behaviour when we are offered alternatives and provided with safe spaces to learn how to adopt them.
It is also important to highlight the huge variation in responses to ACEs. For one child, a single adverse event can be profoundly disabling, less so for another. Part of this is the availability of resilience factors in a child’s life. The value of ‘one good adult’ in a child’s life or a supportive friend, family member, partner for an adult cannot be over-estimated.
Given the high prevalence of ACEs in our culture it is important to recognise that self-care is not selfish – we need to look after ourselves to be there for others.
* A general population survey in Wales showed 47% with at least one ACE. Those with four or more ACEs are more likely to have been in prison, develop heart disease, more frequently visit the GP, develop type 2 diabetes, have committed violence in the last 12 months or have health-harming behaviours (high-risk drinking, smoking, drug use). www.healthscotland.scot/populationgroups/children/adverse-childhood-experiences-aces/overview-of-aces
Reference
Felitti VJ, Anda RF, Nordenberg D, Williamson DF, Spitz AM, Edwards V, Koss MP, Marks JS (1998) Relationship of childhood abuse and household dysfunction to many of the leading causes of death in adults the adverse childhood experiences (ACE) Study American Journal of Preventive Medicine, 14(4), 245–258.






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}