
A simple model to find patient hope for positive lifestyle changes: GRIN
Jen Unwin, Clinical psychologist
David Unwin, GP
Published in JHH16.2 – Faith, hope, love in healthcare
We work together in a GP practice to bring psychology into the GP realm.We realised that psychological theory can seem complex and time consuming to translate into general practice. However, a large proportion of consultations are for physical and mental health conditions exacerbated by behavioural/lifestyle factors such as smoking, alcohol consumption, inactivity and poor nutrition. Doctors often lack the confidence and competence to address these issues in clinic, assuming a lack of patient motivation or fearing opening a can of worms in an all-too-short consultation.The result can be worsening wellbeing, repeat consulting and poly-pharmacy. We have devised a simple four-step plan that we have been using in 10-minute GP appointments for more than 15 years. It enhances the hope that people have for achieving their personal goals and hence their ability to make significant and lasting positive changes in their wellbeing and health. Specifically it is part of an approach that has helped us achieve drug-free remission for 57 people with type 2 diabetes, along with significant practice drug budget savings (Unwin and Unwin, 2014)
He is the best physician who is the most ingenious inspirer of hope.
Samuel Taylor Coleridge
Hope is what makes us strong. It is why we are here. It is what we fight with when all else is lost.
Pandora
The importance of hope
Hope has been defined as the belief that pathways exist towards our desired goals and that we have the motivation and skill to pursue those pathways. Hope is the belief in a preferred future. A positive psychology researcher, Charles Snyder (2002), summarised the research in this area. Hope is a major component of well[1]being and adjustment to adversity. High hope individuals have greater self-reported wellbeing and health. They are actually less likely to get ill and cope better if they do (Unwin et al, 2009; Billington et al, 2008). They consult less. They even live longer. Hopeful people are happier and happy people do better on a whole range of metrics related to health and wellbeing (Diener and Chan, 2011; Unwin and Dickson, 2010).
Perhaps that is not too surprising. However, what is surprising is that the powerful effects of hope on wellbeing are so rarely harnessed in healthcare settings. In fact, it is often the exact opposite. Consultations focus for the most part on what is wrong with people (symptoms) and possible risks to health. This negative emphasis can result in greater patient anxiety, unnecessary prescriptions and tests that do not lead to enhanced patient self-efficacy but instead increase learned helplessness.
Another way to understand the importance of hope is to look at research into the power of the ubiquitous placebo effect. The placebo effect is hope in action. Doctors should seek fervently to harness the power of hope in their consultations, by enhancing belief in an achievable preferred future (Frank and Frank, 1993). As a result of focusing on hopeful consultations patients become heroes rather than heartsinks, and clinicians are uplifted and sustained by hearing stories of success on a daily basis (Unwin, 2005).
A simple model to enhance hope: GRIN (Goals, Resources, Increments, Noticing)
Our simple conversational model is based on enhancing hope by using questions from a solution-focused approach (O’Connell, 2012). Solution-focused therapy started as a form of brief family therapy in the US but is now widely used in health, education and business settings.
This approach assumes that people already have the knowledge and skills to move towards their goals or ‘preferred future’ and that the helper’s role is to uncover that confidence and motivation by asking useful questions. The approach we have developed in primary care has four stages that can be pursued in any order but always keeping in view an understanding of the person’s goals or ‘preferred future’. We have used the techniques described in direct patient work, groups and even remote digital interventions to help people with type 2 diabetes achieve significant improvements in control (Unwin and Tobin, 2015; Unwin and Unwin, 2014; Saslow et al, 2018).
Step 1 Goals
The first and most important step is establishing what ‘better’ would look like to the patient
What are your best hopes for our consultation today?’
‘If in six months’ time, things were how you wanted them to be, what would that look like?’ ‘
Are there any particular ways you would like your health to improve
Usually people will come up with concrete goals such as ‘I want to breathe better’ or ‘I want to have no pain in my knees’.
The clinician will then find a rich vein of information, motivation and insight into the person’s values by following this up.
What difference would that make to your life?’
Patients then respond with something of importance to them. For example, someone might say ‘then I can help with my grandchildren more’ or ‘I could keep walking the dog’.
This then allows the clinician to feed back to the patient what they have now learned. For example, ‘It sounds like family is really important to you’. A very useful question in this approach is ‘what else?’ allowing more rich information to emerge.
‘You would be able to keep walking the dog. What else?
Step 2 Resource
The second stage is to explore what is already working in the patient’s life that is going to help them make progress. This enhances the person’s belief in their abilities to make changes. An alternative is to ask for an example from the past, eg ‘Have you ever managed to lose weight in the past? What seemed to work then?
Who is supporting/helping you right now? Or might do so?’ ‘
What helps your now? When are things even slightly better?’ ‘
What has helped you in the past?’ ‘What personal strengths do you have that could help?’
‘What else?’
Sometimes the strengths question is difficult for people to answer. A different slant can be to give the person a sincere compliment based on what you already know of them, or to ask what a loved one would say.
I know you are a very determined/organised/ positive/caring person and that this will help you to make good progress.’ ‘
What would your wife/best friend say are your best qualities?’ ‘
What else?’
Step 3 Increments
So many people have goals they never realise because they fail to take those first small steps towards their goal. So the third stage of the conversation is either about what would be happening if the person first started to make progress and what they might notice when they do, or committing to some specific ‘small steps’ they think would be helpful.
What will be the next small sign that you are making progress?’
‘What will your wife/best friend notice that will tell them you are making progress?’ ‘
What will tell us you are making progress?’ ‘Bearing in mind your goal, can you think of a small change you can easily make before we meet again? ‘ ‘
What else?
This last question can lead to permission for regular measurements and tests such as waist circumference, weight, BP or HbA1c, for example.
Step 4 Noticing
So often the medical paradigm is about noticing negative things like pain or depression and asking how bad it is. In this model we are trying to shift the focus to positive experiences by asking what is working and what a person has noticed about any improvement. These questions are very useful at follow-up appointments to keep the conversation ‘progress focused’.
What is better since we last met?’ ‘
What difference has that made to you? Who else in the family noticed?’ ‘
What seems to be working well for you right now?’
‘What else
The healthcare professional should also be attuned to noticing progress and giving positive feedback.
I have noticed that you are smiling more/came without your stick/are breathing better this week.’ ‘
Your tells me that you have been successful in making important changes…’ ‘
Wow! You have lost 3″ off your waist. How did you do that?’ (get details)
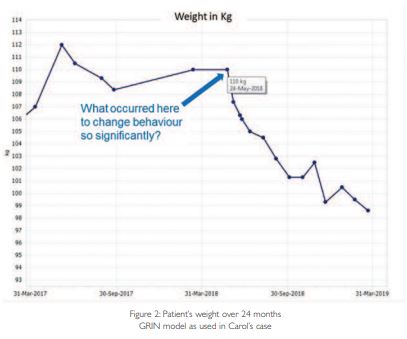
We have found that patients respond really positively to graphs of progress printed from the EMIS GP computer system (see example below) and like to show family and friends how much progress they have made. In a nutshell noticing supplies feedback.
GRIN case study (based closely on a patient of David’s, with consent)
63-year-old ‘Carol’ went through the practice diabetes screening programme and was found to have a raised HbA1c of 46 mmol/mol (NR
Patient’s individual health Goals On being asked:
‘Carol, in general what would you most like to see improve in your health?’
She answered: ‘To be able to breathe better – I get really scared at times.’
Note that she was not really interested in her raised HbA1c – that just made her even more worried. Instead it was better to pursue a positive, more solution-focused line by asking: ‘
If you could breathe better what difference would that make to your life?’
She answered: ‘Well, it would be so great to worry less about my breathing – sometimes I wonder where this will all end…’
Next question: ‘
What else would be better if you could breathe more easily?’
She replied: ‘
I help look after my three-year-old grandson and I would love to be able to be more active with him, he’s so lively!’
Note that the tone of the consultation improves as we move from fears to hopes.Also, the more someone adds detail to a preferred future, the more likely they are to believe in it and want it. My next question would be around what activities breathing better might allow her to share with her grandson.The more she inhabits a preferred future the more likely she is to make the necessary changes to achieve her goals.
Only then will I ask:
‘In your experience what might help you breathe better?’
Note we are still not talking about my goal around the HbA1c because it’s not hers. But with patience we will get there. I am trying to find a shared goal.
Her response: ‘
Well it’s obvious I need to lose weight, stairs are a nightmare for me!’ Bingo!
Resources
It’s important to resist the urge to give advice before further exploring the strengths and wisdom your patient already has.
‘If you have ever lost weight before what has helped you succeed?’ ‘Being organised seems to help me, getting the fridge ‘sin free’ for a start.’ ‘What else?’ ‘Also, I’m quite a fan of social media so I found some good.
Increments
So many of us have a grand scheme but those first steps towards a goal are the most important.
Carol can you think of something you can commit to right now, today, to help you lose weight? ‘ ‘
Really I suppose in view of the diabetes thing the nurse mentioned, the biscuits and cake should be the first to go.’
Now at this point some strong reinforcement can help, perhaps discuss exactly how this is to be achieved and agree a next appointment to re-weigh and see how it’s going.
‘What a great idea! What do you hope to be telling me in two weeks’ time? How will you/I/your family know this is working well?
Noticing
Sometimes we wonder if this is the most powerful part of positive psychology. Noticing both what works and crucially what feels better seems to be central to further success.The classical medical paradigm is the opposite of this, focusing as it does on symptoms of disease like pain or depression.The only way to get a doctor’s attention is to moan louder! Perhaps in this way, we make not just the patients but ourselves more miserable. In this case Carol agreed to be weighed again after three weeks. Looking at the graph in Figure 2 you can see she had lost an amazing 2.8 kg.
Carol that is amazing, well done! I’m really interested – have you noticed any other improvements yet?
Yes my family say I’m more cheerful – it feels good to be more in control and I didn’t miss the biscuits as much as I expected.’ ‘What else?’ We see noticing as closely related to feedback, an important part of motivation. In Carol’s case printing off her weight graph supplied more positive feedback as I could point out she was the lightest she had been for over a year
That completed this GRIN cycle;
now the process can be repeated to build on her success.
‘Right Carol that’s biscuits and cakes beaten, what’s your next goal?’ ‘
I was wondering if perhaps I eat too much toast – I know it’s fattening.’
‘You’re right! How will you know when you’ve beaten toast? What will you be eating instead?’
It’s been a year now and Carol has lost more weight than ever before in her life.The two transient blips on her graph are due to courses of steroids for her asthma, but she didn’t end up in hospital once over the winter. She is pleased to notice it’s not just that she breathes better but she feels healthy. ‘
What else is better?’
‘My family are so proud of me! Oh and I buy smaller clothes now. And you know I don’t miss bread a bit, and yes I can bend over to play with my grandson easily these days.The best bit is to feel less scared and more in control of my own health!’
What about that raised HbA1c? It’s now 41mmol/mol, (in the normal range).This makes the point of how holistic a hope-based, patient-centred approach can be. Carol’s blood pressure is better too.
It is also worth noticing how this process affected me as her doctor. I have looked after Carol for more than 30 years, but it’s only in the last year that I have noticed what a resourceful, determined person she is. I feel it’s a cheat that she is so grateful to me because it has been her efforts that have made such a difference.These days I look forward to hearing how she is getting on. Cases like this give hope and energy back to the doctor and can improve healthcare professional resilience.
We mentioned using this approach in 10-minute appointments.We called it GRIN to help people remember the four components but in pressurised clinical practice it is fine to use any one or two of the four in a consultation. For instance, in a case with multiple morbidity, if all you manage is to explore your patient’s health goals or relevant resources your time is well spent. Practitioners who are new to this might have the goal of using a minimum of one of the elements in each case.A useful training exercise is to see how many times in a morning clinic you can give out a sincere compliment then notice how that affects your patient interactions.
Wider application of the mode
The process of shared goal setting, acknowledging what is already working, identifying the next steps and noticing progress is a simple model that can also be applied to meetings, supervision, appraisal, family and personal goals.
What are our best hopes for this meeting today?’
‘Where do I/we hope to be this time next year?’ ‘
What is already going well in our team?’ ‘What strengths do we have in the team?’
‘What will tell me I am managing you better?’
‘When have I noticed myself being at my best recently and how did I do that? ‘ ‘
What have I/we been pleased to notice in the last week?’ ‘
What else?
Using a solution-focused approach challenges the traditional model that any problem must be understood and analysed in detail before progress can be made. It gets away from ‘diagnosing’ the problem to envisioning the solution. Most clinicians believe that taking a history detailing the causal events that led up to illness is always important in finding the remedy. In fact, though this may help understanding, sometimes it can hamper progress. For example, patients may have experienced extremely difficult childhoods but examining the details of just how traumatic can sometimes lead to people feeling worse. In a case like this, particularly if time is short, an alternative could be to notice resilience with a sincere enquiry about ‘toughness’ by asking, ‘that sounds so hard, I’m interested to understand how you managed to get through those difficult times?’ This may be an excellent prelude to exploring goals, and a much more productive and cheerful use of time than taking your patient through a very painful, detailed examination of half-buried trauma. In this way progress can be fast and sometimes surprisingly so. Practitioners must be ready to give up ‘advice’ and have faith in the patient’s expertise and strengths. The practitioner’s knowledge and experience is then used to support the patient’s efforts and progress.
We have found this approach to be easily incorporated into a wide range of clinical scenarios. It is positive, patient-centred and less burdensome on staff. Surely, this is much needed in helping both patients and staff remain happy, resilient and well.
References
- Billington E, Simpson J, Unwin J, Bray D, Giles D (2008) Does hope predict adjustment to end stage renal failure? British Journal of health Psychology 13 (4) 683–700.
- Diener E, Chan M (2011) Happy people live longer. Applied Psychology: Health and Well-being 3 (1) 1–43.
- Frank J, Frank J (1993) Persuasion and healing. Baltimore, MA: John Hopkins University Press.
- Malpass T (2018) The hope that I have: to remission and beyond. Print2Demand. print2demand.co.uk.
- O’Connell B (2012) Solution-focused therapy. London: Sage Publications Ltd.
- Saslow L, Summers C, Aikens J, Unwin D (2018) Outcomes of a digitally delivered low-carbohydrate type 2 diabetes self-management program. JMIR Diabetes, 3 (3) e12.
- Snyder C (2002) Hope theory: rainbows in the mind. Psychological Inquiry 13 (4) 249–275.
- Unwin D (2005) SFGP! Why a solution-focused approach is brilliant in primary care. Solution News 1 (4) 10–12.
- Unwin D, Tobin S (2015) A patient request for some ‘deprescribing’. BMJ 351 h4023.
- Unwin D, Unwin J (2014) Low carbohydrate diet to achieve weight loss and improve HbA1c in type 2 diabetes. Practical Diabetes 31 (2) 76–79.
- Unwin J, Dickson J (2010) Goal focused hope, spiritual hope and well-being. Social Scientific Study of Religion 21 161–174.
- Unwin J, Kacperek L, Clark C (2009) A prospective study of positive adjustment to lower limb amputation. Clinical Rehabilitation 23 1044–1050.






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}