

Healthcare system transformation coupled with optimising individual and population health and wellbeing
Campbell Murdoch, GP
Published in JHH13.3 – Saving the NHS
My role as a GP has, over the last three years, been one of enthusiasm and energy – truly! Having studied medicine in the late 1990s the ‘evidence-based medicine triad’ and the ‘bio-psycho-social model of health’ became firmly tattooed onto my conscious mind. Later I undertook postgraduate studies in teaching, organisational behaviour, leadership and also sports and exercise medicine.This has provided me with a perspective and toolkit to use with my fascination of understanding what it is to be human, and how in our complex and resource-limited world human health and wellbeing can be optimised in the most effective way.
[bctt tweet=”The GP remit has shifted over the last few decades towards also managing chronic diseases and disease prevention” username=”BritishHolistic”] Humans are diverse, multifaceted beings living in an ever-changing world. A dynamic adaptive approach to healthcare is what we need in order to interact effectively with such complex dynamic interdependent systems. The linear medical model, which can be very effective in some acute medical scenarios, is often inadequate or ineffective for the many individuals who present with more complex and chronic health and wellbeing needs.
The GP remit has shifted over the last few decades from mainly providing solutions or interventions to acute conditions, towards also managing chronic diseases and disease prevention. This transformation is driving a fundamental shift of focus towards whole person and whole population healthcare. If it can be shown that this new approach is more effective and efficient than the narrower focus on biomarkers alone, then optimisation of individual and population health and wellbeing could be achievable even within current resource constraints.
However, up until now we have transitioned the old linear fix-it medical model into arenas for which it was not designed. There are many reasons for this: an innate desire for simple solutions, reductionist thinking, market-driven healthcare, and the usual human tendency to stick with the things we are used to. Even though we have become very good at targeting some culprit disease biomarkers, our interventions will be ineffective at best and could at worst be harmful if the targets are the wrong ones.
I believe that we are about to experience a re-humanising of the healthcare system. There are strong drivers for this shift, not least the need for a more financially sustainable system. But behind it too are personal human drivers: the declining morale of many who work in healthcare services and their general desire to do good for their fellow humans. Could it be that a simple, flexible shared paradigm of health and wellbeing, acceptable to most users, could bring about solutions in all three areas? Might it be possible in one fell swoop not only to make far better use of our limited resources, but at the same time support more humane practice and meet today’s complex needs?
Some primary care history: the QOF
The UK Quality and Outcomes Framework (QOF) was first rolled out in 2004. With the desire to drive up universal standards of care – and enabled by the mass adoption of electronic medical records – GPs were rewarded for hitting certain quality targets. The QOF definition of prevention was for the most part confined to testing for certain biomarkers – for instance blood pressure, cholesterol, blood glucose – and prescribing appropriate drugs to control them. Unfortunately, in practical terms, there are still relatively few biological factors we can meaningfully measure and record. And so, in the drive to practice ‘preventative medicine’, and even though impelled by the new GP contract, ‘the best available evidence’ for producing useful quality markers for prevention fell short of what was really needed to make the QOF fit for purpose . Yet over the next decade, the focus on QOF-driven primary care shifted general practitioners’ focus away from doing what they might formerly have felt was best for the individual in front of them, because they had been incentivised to prioritise doing things intended to be good for whole populations.
Although, QOF helped standardise medical practice and may even have driven up efficiency, I believe it unwittingly reduced the effectiveness of care provision. A prime example of how immense resources can be efficiently applied but be relatively ineffective in achieving true health benefits is the use of statins. With the laudable aim of preventing future cardiovascular disease, GPs were financial incentivised to focus on total blood cholesterol levels, and the imperative to reduce them with medication.
In practical terms, there are still relatively few biological factors we can meaningfully measure and record
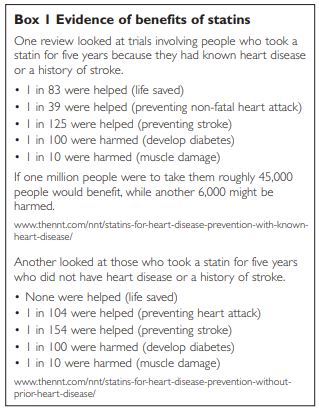
This QOF target leveraged huge resources for a healthcare intervention of questionable benefit, since the evidence for statins at population level is neither clear nor universally agreed upon [see box 1]. In this particular case, targeting a single biomarker misapplied the linear medical model of acute medicine to a complex multidimensional condition, because the likelihood that a statin will benefit an individual – even someone who has cardiovascular disease – is in fact rather small, as can be inferred from the numbers needed to treat statistics in Box 1.
The next step in the evolution of healthcare
In Somerset in 2013, just under a decade after QOF’s advent, there was a growing awareness that the healthcare system was not meeting people’s needs. There were many reasons for this, among them an ageing population, and a net reduction in the healthcare workforce. It was becoming clear that if the healthcare system was going to evolve into something more effective and viable, primary care would need the freedom to divert resources into areas where it could have real impact. But only by unshackling it from the QOF would primary care be able to innovate and adapt. In fact if individuals’ health and wellbeing needs were ever going to be met the entire health and social care system would have to engage in new models and paradigms of working with Somerset’s population. Discussions between NHS England, the Somerset Clinical Commissioning Group and the primary care workforce produced an agreement for GP practices to opt out of the national QOF and into an alternative scheme named Somerset Practice Quality Scheme (SPQS). What we were looking for was an environment that could enable organisational and system transformation. Through the design and various mechanisms of SPQS (which are not discussed in this article) primary care can start this journey. The destination will be a mature, collaborative primary care system, functioning as a high quality learning organisation able to better align its resources to Somerset’s needs.
Evidence-based medicine was originally meant to take into account not only the best available research evidence but also the person’s wishes (and expertise) and the professional’s skills and knowledge. If SPQS helps us achieve this transition it will have been a revolutionary success. But already, on a personal level moving from QOF to SPQS has been truly transformational. Instead of existing in a constrained and inflexible system I found I could use my energy to make primary care more effective and efficient. Whereas the QOF had put my purpose and my passion for medicine at odds with my need for an income (by incentivising me, for example, to chase cholesterol reduction with drugs in an 85-year-old while pushing me to ignore her loneliness) I was now able to focus on what makes me want to get up in the morning, go to work with integrity and strive to optimise individual and population health and wellbeing.
The Human Five is helping to provide a number of solutions in primary care
The Human Five – a universal health and wellbeing model
SPQS allows me to focus a dynamic approach on complex dynamic situations. I no longer have to be blinkered and see people as simply diseases, I am free to see myself and each person I meet as a unique human being. This may sound rather subtle, but I can tell you that the difference it makes is extremely powerful!
Given this new freedom to innovate and adapt, we developed an idea that is now helping shape the way we provide healthcare: a simple universal health and wellbeing paradigm called The Human Five. The Human Five is helping to provide a number of solutions in primary care. It is based on a paradigm that enables people – doctors, health coaches, social care workers and others in the community – to work together, by encompassing as it does the spectrum of individuals’ health and wellbeing needs. It also provides a framework for thinking about population health. The assessment/ consultation tool itself, which can easily be integrated into everyday primary care work, may be used explicitly when working with a patient or just kept in mind as a loose framework for shaping better consultation. (The assessment/consultation tool can be found on page 31 and I hope practitioners will find it useful.)
Case scenario: QOF consultation vs SPQS consultation
I have written this vignette to reflect a real-life GP scenario. I hope it illustrates the profound effect of changing the primary care consultation paradigm and environment. It is intended to highlight the contrast between QOF-oriented practice and the kind of primary care consultation made possible by SPQS.
It is 7.30 in the evening when Mrs Evelyn Jones arrives for her appointment. You don’t know her but can see from her notes that she is 78 years old and recently had her annual hypertension review with the nurse. Her blood pressure was 155/80. Her blood tests from the review have arrived back. You also see from the notes that she had a bereavement a month earlier.
Scenario 1:A QOF consultation
After a quick scan of Mrs Jones’ medical record you call her in, welcome her and ask why she has come. She tells you: ‘The nurse told me my blood pressure was too high’. You reassure her that ‘Yes it’s higher than ideal, as it’s best kept below 150 for the top number’. Mrs Jones asks, ‘Is it at a dangerous level doctor?’ You explain, ‘There is no immediate danger, but high blood pressure can raise your risk of having a heart attack or stroke. So we aim for the top number to be less than 150 for most people’. You ask her, ‘How are you getting on with your current medication?’ She is on two medications to lower her blood pressure.’Fine I think.’ she replies.
You are not dreadfully keen to add a third anti[1]hypertensive. You suggest to Mrs Jones that you recheck her blood pressure now. As it’s a cold evening Mrs Jones is wrapped up in a number of layers. She stands up to take off her long coat, and as she does so you notice she’s probably got some arthritic joints in her legs. After a few minutes of layer removal there is upper arm skin exposed ready for the blood pressure cuff. You take her blood pressure – the first reading is 158/86, and the second reading a minute later is 153/78. Mrs Jones asks, ‘What’s it like now?’ You advise her its a little better, but not quite at target. Mrs Jones looks at you impassively.
You are nearing the end of the consultation time. You have a nagging awareness that the QOF end of year is not far off. If you don’t ensure Mrs Jones’ blood pressure is recorded at being below 150/80 by the end of March you could lose QOF points (and thereby personal income). So you decide you had better add a third blood pressure tablet now so there will be time for Mrs Jones to get back in a couple of weeks and have the nurse repeat her blood pressure: hopefully it will be under 150/80 by then.
You prescribe Mrs Jones amlodipine 5mg. ‘This should help lower your blood pressure some more.’ Mrs Jones looks a little sad. ‘Does this tablet cause any side-effects?’.
You tell her, ‘The commonest is swollen ankles’. Mrs Jones looks down at her ankles which you can see are already are a bit swollen. ‘They normally get puffy by the end of the day already.’ You ask, ‘Do they go down overnight?’ She replies, ‘Yes they’re fine first thing.’
You have another fatigue-fuzzed internal debate – QOF targets, income, lower blood pressure, swollen ankles, dependent oedema or heart failure? Maybe amlodipine is not such a good idea after all…. You are now overrunning by five minutes. So with this in mind and needing to get to a resolution you decide. ‘Well you might well be fine with 5mg of amlodipine, give it a go, we’ll review it and we can always stop it again.’
You start to prescribe the amlodipine and remember that her blood tests are back (renal function, HbA1c, and blood lipids including her total cholesterol level which is 5.2). You see that she currently takes simvastatin 10mg. You are now rushing, but QOF is on your mind, the total cholesterol target for QOF is <5. You know that using total cholesterol levels as a marker of risk of future ill[1]health is not reliable, but you also know you could probably get Mrs Jones’ total cholesterol level below 5 if you increased her statin to 20mg.
You say: ‘Your cholesterol level is up as well. I’m going to increase your dose of simvastatin’, as you hurriedly print out a prescription for amlodipine and the higher dose of simvastatin without making eye contact with Mrs Jones. You hand the prescription over along with a slip to give to the receptionist. ‘Here you go, take this to the receptionist who will book you for another blood test and blood pressure check in a few weeks. Do let me know if you have any problems.’
Mrs Jones thanks you and gets up unsteadily from her chair. You help her on with her long coat and guide her out of your consulting room. You dash back to your desk to quickly type up the consultation notes in her medical record. In your fogged and fatigued mind you quietly question what benefit that consultation did for Mrs Jones’ health and wellbeing. No social issues were raised by Mrs Jones; in some ways you are relieved as the consultation took too long anyway. You briefly wonder what her recent bereavement was all about. But the thought is a fleeting one and as you call the next patient in 10 minutes late and thank them for waiting, it soon fades from your mind.
Scenario 2: SPQS consultation
Quick scan of Mrs Jones’ medical record. You call in Mrs Jones and welcome her into your room. ‘I’m Campbell Murdoch, I don’t think we’ve met before but it’s good to meet you. What is it we are doing this evening?’ Mrs Jones says the nurse had suggested she comes in to discuss her blood pressure which was apparently a bit high at her annual review.
You have a glance at her records and respond, ‘Okay, well it’s a little higher than your normal but blood pressure can go up and down very quickly, within seconds or minutes, it can also increase when life changes happen.
And the good news is your blood pressure is certainly not causing any immediate dangers.’
You recall the ‘bereavement’ code in the problem list in her medical record and ask, ‘How are you in yourself at the moment?’ Mrs Jones looks at you and says, ‘Life’s been difficult, my husband died a month ago, do you remember him, you came to see him a couple of years ago?’ You don’t recall meeting her husband but are saddened by the news and the likely impact on Mrs Jones. You say, ‘I’m very sorry to hear that. How are you?’ Mrs Jones replies, ‘I’m doing okay. My daughters have been good but they’ve had to go back now, they live away and have their own families and work to deal with.’ You acknowledge Mrs Jones’ comments and feel you should close the blood pressure issue so that it is not a nagging concern. You say to her, ‘That sounds pretty tough for you. It certainly would explain why your blood pressure was up a little, and that’s okay, blood pressure is supposed to do that. What are your next few weeks at home looking like?’
Mrs Jones looks sad but is maintaining eye contact with you and states, ‘Well, my daughters are coming down at the weekend again to see me. They’re worried I’m lonely, I would have been married to Bill for 60 years next week and we did everything together. They’re going to take me out for a meal.’
You are pleased to hear that Mrs Jones has daughters who care about her and are in touch, even if they don’t live locally. You perceive that Mrs Jones’ social situation will change significantly over the coming weeks, months and years.
You say to Mrs Jones, ‘Well, enjoy you meal with your daughters this weekend. Do let me know if we can do anything here at the health centre to help. We have some extra staff here now who can give you some support if you would like it. Vicky, a health coach, would be very keen to meet with you if you would like. There are lots of support groups in the community too, which she could help you get involved with if you’d like. Just call the practice and ask for Vicky. Either way you are very welcome to come back and see me over the coming weeks if you want. And at some point in the next few months we can check your blood pressure again, but it doesn’t need to bother you at the moment.’
Mrs Jones replies, ‘Thanks doctor, I’ll do that’.
You quickly glance at her medical record again and scan her blood test results. Your eye is drawn to her blood lipid results. You feel deeply relieved that you now do not have to wrestle with conflicted thoughts of whether you should increase Mrs Jones’ statin dose to lower her total cholesterol level.
You help Mrs Jones on with her coat and guide her out of the consulting room with a smile.
You dash back to your desk and quickly write the consultation notes in her medical record. Even though you’re tired from your busy day you have a sense that you may have just improved Mrs Jones’ wellbeing. You call in your next patient five minutes late and thank them for waiting.






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}