

Connecting citizens and services in new and meaningful relationships to transform healthcare
Alyson McGregor, Director of Altogether Better, an NHS National Network Organisation
Published in JHH13.1 – Shaping the invisible
After spending many years working very hard in the NHS doing the wrong things well I was lucky enough to become the director of Altogether Better and became part of a network of people who helped me discover what really matters.Working alongside a group of health leaders, doctors, academics, organisational development consultants, social activists and citizens I have learned that almost everything we do depends on other people and that to succeed we need to work as peers, as equals, valuing the contribution of others and working out solutions together.This means that we need to pay attention to the relationships we have with others and to focus on our connectedness.This learning underpins not only the way we work but our whole way of being in the world. It allows us to see the world as resourceful and abundant and full of amazing possibilities.
[bctt tweet=”The nature of disease has changed fundamentally… we live in an age of diseases which are largely social” username=”BritishHolistic”]
Introduction
The NHS is no longer sustainable in its current form as it struggles with the emerging challenges of an increasing burden of long-term conditions and health needs generated by social factors such as isolation. The morale of staff in general practice is low, as pressures in the system increase and funding is unlikely to match escalating demand. Equally we are not serving the populations needs well; people with long-term conditions are not getting the support they need and a session with the GP can’t ‘cure’ isolation.
In response, the NHS Five Year Forward View (www.england.nhs.ukk/ ourwork/futurenhs) asks us to imagine new models of care and ‘a future where fully engaged patients, carers and citizens play a greater role in their health and health care’. It argues that health services need to change, and develop a more sustained relationship with patients, carers and citizens. But there are few examples where citizens have made a significant change – through participation rather than consultation – to the way that general practice and wider health and social care services are designed and delivered.
This policy backdrop echoes Altogether Better’s vision for an NHS where citizens are recognised as part of the solution and not the problem and where citizens gift their time, talents and enthusiasm to work along[1]side primary care workers as equal partners. Using a systems model of organisational development and an evidenced-based health champion approach to citizen involvement, we prototyped and scaled a radical system-intervention which slowly, gently and subversively allows the practice and the population it serves to co-evolve.
‘We have increased our patient list by 4,500 people, that’s a 57% increase, and we have seen no increase in demand for either primary or secondary care consultations because we do things differently.’
Mev Forbes, Managing Partner, Robin Lane Medical Centre
This new relationship and connected[1]ness between citizens and services leads to the emergence of a vast range of new offers that promote wellbeing and resilience, prevent ill-health, and treat people who struggle to live well with their long-term conditions, isolation and loneliness. We have worked with GP practices and citizens to create a future where general practice is drawing on the assets, strengths and resourcefulness of people in their communities as well as the staff in their services, to do things differently and find new solutions to the pressing and overwhelming pressures faced by healthcare services.
The overwhelming case for change in general practice
The kind of data needed to provide us with the whole picture about what patients present with in general practice is not routinely collected. However, it has been estimated that around 20% of patients who consult their GP bring what is primarily a social problem. In fact the Low Commission (2015) reported that 15% of GP visits were for social welfare advice alone. This may well be a huge underestimate, for many GPs anecdotally report much higher levels of demand. Far from addressing this need, increasing the number of appointments or extending opening hours will only make things worse.
My estimate is that 40–55% of the patients I see every week could be better supported by someone else, they don’t need to see someone with five degrees. It’s a rotating door; they just come back again and again. Patients need people not pills.’
Dr Niall Macleod GP, Exeter
Dr Niall Macleod, an Exeter GP, estimates that:
- 10–15% of people come with minor ailments – sore throat, headache, that could be sorted by a pharmacist or a wise granny
- 10–15% of people he sees are depressed, anxious, stressed, fatigued. They need a job, friends, a loving partner, NOT anti-depressants or counselling
- 10% are overweight and have lifestyle-related issues type 2 diabetes, hypertension, heart disease. They need to lose weight, move about more, eat fresh food. NOT blood pressure tablets
- 5% are lonely and the GP is the only social contact
- 5–10% are just getting old! They have lots of problems and there is no cure.
For these patients to medicalise their problems is inappropriate, results in over-diagnosis and is equally frustrating for both patient and GP. GP training places remain unfilled, senior GPs are retiring early and insufficient numbers of junior doctors are applying to join general practice because of a perceived impossible workload.
And it’s not just GPs who are affected by the current pressures in healthcare. Healthcare professionals generally work tirelessly to do their best for patients in the face of ever increasing workloads.
Stumbling upon a new model of general practice
Responding to this crisis Altogether Better developed and spread a system intervention that has allowed GP practices and the population they serve to co-evolve, creating a movement towards a social model of primary care which could in turn lead to a more sustainable primary care system. The evidence tells us that when this approach works well, it leads to an NHS where:
- a new social model of care emerges within general practice which effectively reduces demand on GPs’ time
- consultations in primary and secondary care reduce
- a new sustainable business model for general practice emerges
- staff morale improves
- we learn ways to connect and work together with people, not do things to them or for them
- people in communities connect effectively with and work alongside staff to become part of the practice ‘family’, thus breaking down unhelpful and outdated hierarchies
- patients get what they need and not only what professionals can offer.
Our model started to take shape in 2012 when, combining theoretical models of organisational development and our evidence-based, health champion approach to citizen engagement, we created an innovative approach to ‘community centred practice’ in three GP centres. The impact of this was encouraging enough for us to explore how to scale up the work. We then developed and spread this approach to more than 60 practices, in 16 clinical commissioning group areas, by working nationally and internationally with enthusiastic practices where citizens were invited to work alongside staff. We are noticing that when the right conditions are created, practices begin to see citizens as ‘makers and shapers’ in the system rather than ‘users or choosers’ who pass through it. They begin to understand that the community is an asset not a burden.
Failure demand is a systems concept used in service organisations first discovered and articulated by Professor John Seddon as ‘demand caused by a failure to do something or do something right for the customer’. Seddon makes the distinction between ‘failure demand’ and ‘value demand’, which is what the service exists to provide. Failure demand represents a common type of waste found in service organisations.
Wikipedia
We begin by finding GP practices interested in developing a new model of care designed to help them deal with the rising levels of failure demand generated by patients whose health and wellbeing needs can’t be met by a clinical intervention alone.
We support these practices in finding enthusiastic people willing to gift their time to work alongside the practice as volunteer practice health champions. Then we guide and model a way of working together, a way of being connected which works for citizens and for the service.
New service offers emerged from practices including kite flying, conversation club for non-English speakers, bipolar group, fatigue support group, cancer, chronic pain and diabetes groups, ukulele group, circle dancing for patients with dementia, glass painting, crochet and cross[1]stitch. One practice became the first in the country with a licensed bar while simultaneously reducing its primary and secondary care appointments!
We found that having champions as part of the practice changes the nature of the ‘practice family’ so that both groups co-evolve to do things differently. This in turn leads to benefits for patients, champions and the practice. What has emerged is a new collaborative community[1]centred model of general practice.
New relationships between champions and practices become embedded and are sustainable in the long term without ongoing funding. As champions merge into the ‘practice family’ they simply become part of ‘how we do things round here’.
A new mind set
The starting point for the work is the recognition that the NHS is now functioning within an entirely different environment than in its formative years. The nature of disease has changed fundamentally; our healthcare imperatives are no longer driven by the need to fix infectious disease or broken bones. We live in an age of chronic complex multi-morbid diseases which are largely and fundamentally social in character. Demand is provoked by either social factors, such as isolation, diet, poverty, or by an individual’s inability to adapt well to living with long[1]term conditions such as diabetes, asthma or dementia. These impacts are not fixable but neither do they go away. This calls for an adaptive response, a process of coming to terms with their changed circumstances and the need to deal with life differently. These are both social processes, not ‘clini[1]cal’ or ‘professional’, and can be met more effectively with a social response rather than a professional, clinical response. So the challenge for society now is to create systems within which people can adapt and change and achieve ‘health’ which is, as Huber defines it, ‘the ability to adapt and self-manage in the face of social, physical and emotional challenges’
(Huber et al, 2011).
Systems organise around a purpose, and so a way to fundamentally change a system is to get it to identify a new purpose, often by formulating this as a question. The Huber definition helps us shape a new question:
How do we support people to adapt and change in the face of social, physical and emotional challenges?
So health is no longer seen as the absence of disease, and the challenge is to create a system within which people are able to adapt and change. When citizens become part of this changing system the developmental work takes place in liminal space – where neither the rules norms and behaviours of the organisational world nor those of the ordinary social realm applied and would have to be suspended in order for exciting possibilities to be generated.
During liminal periods of all kinds, social hierarchies may be reversed or temporarily dissolved, continuity of tradition may become uncertain, and future outcomes once taken for granted may be thrown into doubt. The dissolution of order during liminality creates a fluid, malleable situation that enables new institutions and customs to become established.
Wikipedia
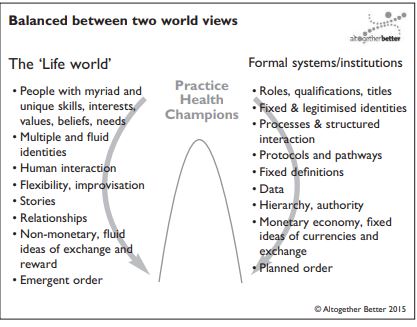
Working in liminal space
Liminal space happens at the boundary between the formal world of organisations and the informal life-world of citizens. Inviting citizens and services to work together towards a new system, we realised unexpectedly that a new world and a new language was being created. It became clear that working at this boundary required a different way of seeing the world, and a new set of skills, norms, behaviours and language, which were all very different from the traditional NHS approach.
…Patients draw strength and resilience from the community… and learn to live well or better
Some people (practice staff and champions) instinctively understood what the work was about. Some struggled. Those who struggled saw it as either an extension of their employing organisation’s way of doing things or they thought it was having a new group of ‘friends’ attached to the organisation/system. Those who understood recognised that it was neither. The closest real life analogy is that of a beach, a place that is neither land nor sea and upon which human behaviour differs from that normally found on either. On the beach, normal rules are suspended and we behave in very different ways for example we dress (undress) and behave in ways that don’t happen elsewhere. Similarly, when connecting and working together in the space between the formal and informal worlds, traditional language and ways of working are no longer effective or appropriate. A major part of the work for Altogether Better was to challenge language and behaviour wherever it slipped out of the liminal space and back into either world, so that champions and practices might come up with appropriate and fit for purpose language and behaviours.
It feels like we’re a GP practice within a larger organisation. There’s the general practice primary care bit which is wrapped around with a much bigger range of things going on.’
Dr Linda Belderson, GP, Robin Lane Medical Centre, Leeds
One of the key lessons was that champions do not receive monetary reward (formal world) but are doing what they do for a purpose; and not just for pleasure. This meant that the practice needed to find different ways to value and recognise the champions. Another theme was the value of sharing tea and cake to strengthen relationships while planning new activities. However, it was equally important that the social aspect didn’t take over and stop effective planning from being done. To connect effectively the conditions need to be created in which the champions don’t just enjoy the experience (lifeworld) or just get the task done (formal world), but enjoy both the process and the end result of making a difference.
What grew out of this new understanding of working in liminal space could not have been predicted. Citizens, joining this work as volunteer Champions who had been invited by their practice to work with them, drew on their own passions, interest and resourcefulness to generate an enormous range of groups, activities and events for the patient list. A comprehensive evaluation, which drew on evidence from the government’s Foresight Project and the New Economics Foundation, demonstrated that 216 different champion-led activities brought about improvements in patients’ wellbeing and resilience and a better understanding of how and when to use services. This increased resilience in turn leads to an ability to adapt, cope and live well with long-term conditions. In other words, patients draw strength and resilience from the community – ‘people like me’ – and learn to live well or better, adapting to the ever-shifting challenge of health concerns that cannot be ‘fixed’ by clinicians. With over 15 million people in the UK living with one or more long[1]term condition, this work could not be more timely.
A new model of systems-working
This work is not social prescribing in the usual sense of shifting the burden from one professional (GP) to another (third sector providers). Nor is it for creating new referral pathways whose starting point is still the doctor’s or nurse’s consulting room. It is not ‘signposting’ or a means of parachuting volunteers into a practice setting. It requires both a shift of mindset and a slightly different way of organising. So unsurprisingly these changes don’t happen without skilful support. The biggest threat to scalability of this approach would be if system leaders, GPs and practice managers failed to take the time to understand what is radically (but subtly) different about our approach and so default to framing it merely as a volunteer programme.
94% of patients surveyed reported increased confidence and wellbeing
Our evidence is growing and compelling, and our approach to ‘community centred practice’ has gained national and international recognition. Forward thinking practices and commissioners are pulled towards it, recognising it as one of the solutions to the challenges faced by primary care teams under huge pressure. When enthusiastic practices and champions work together we see significant improvements in mental health and wellbeing and overwhelming support from practice staff to embed and sustain the work:
- 94% of patients surveyed reported increased confidence and wellbeing
- 94% acquired new knowledge about health and wellbeing
- 99% reported increased involvement in social groups and activities
- 95% of staff surveyed recommend and want to continue the work.
A case story from Robin Lane Medical Centre, Leeds: Creating a sustainable future for general practice
We had a growing realisation that general practice was unsustainable in its current format. We knew that funding was going to be an issue. We can’t just go on employing more and more doctors to meet more and more demands, we had to think quite radically about how to change demand in the first place.’
Mev Forbes, Managing Partner
Robin Lane now works with more than 50 enthusiastic citizens who deliver 19 different kinds of groups and activities. As well as the plethora of champion-led social groups, the practice now runs a Ukulele group, provides 7 day a week breastfeeding support delivered by champions, keeps a constantly updated dynamic directory of local services and resources and signposts and routes people to activities in the community.
Champions also support service delivery in many different ways including for example increasing the number of people attending Saturday flu clinic from 300 to over 800 people.
‘The champions have enabled a lot of things to happen which wouldn’t have been able to happen otherwise’ (Linda Belderson, GP). ‘But the great story is that lives have been transformed, people are no longer isolated; they have made new friendships and use services differently’ (Mev Forbes, Managing Partner).
Evidence of improved efficiency and increased productivity:
- The practice has increased its patient list by 57% from 8,500 to 13,000 patients without any increase in primary of secondary referrals and a 10% reduction in use of A&E
- There is evidence of increased efficiency by dealing with failure demand
- Over 50 volunteer practice health champions work alongside the practice team
- The practice has reconfigured its staff team and redesigned its offer to respond to the new challenges, choosing not to appoint to a vacant salaried GP post but instead choosing to invest in a community matron and a wellbeing co-ordinator
- The practice has evolved to do things differently – its identity has changed. It no longer describes itself as a medical service and is rebranding as the Robin Lane Health and Wellbeing Centre.
Reference
- Huber et al, BMJ, 2011 How should we define health. BMJ 2011;343:d4163 doi: 10.1136/bmj.d4163 The Low Commission (2015) The role of advice services in health outcomes: evidence review and mapping study. Available at: www.lowcommission.org.uk/dyn/1435582011755/ASA-report_Web.pdf (accessed 12 March 2016)






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}