
The star of compassion
Eleanor Tanner, Medical student, University of Birmingham
Published in JHH12.3 – Beyond Peak Medicine?
I am a final year medical student at the University of Birmingham. I am particularly interested in paediatrics and loved my placement at Birmingham Children’s Hospital. I have also enjoyed a variety of activities working with children outside university, including regularly working with a young boy with autism.This has highlighted to me the importance of considering each individual’s needs. I also work shifts in a nursing home to broaden my experience across the age spectrum. I have experience as a carer for family members and as a patient myself; I aim to use all of this to enhance my understanding of patients I encounter.
‘Compassion’ is often cited as an essential characteristic of a holisticfocused practitioner (Gelhaus 2012), and indeed prospective students attempt to prove this quality to gain entrance to medical school (Shakespeare 2013; Leget and Olthuis 2007). ‘Compassion’ derives from the Latin ‘to suffer with’ and the Oxford English dictionary defines it as ‘sympathetic pity and concern for the sufferings or misfortunes of others’. The disability movement would regard ‘pity’ as patronising, oppressive and disempowering (Lang 2007). However, compassion is far deeper, reaching into the heart of human emotions. It incorporates empathy, kindness, and the devotion of one’s time, energy and emotions to the needs of another. Healthcare professionals (HCP) by definition provide ‘care’ for patients, but caring ‘for’ someone is not the same as caring ‘about’ them. True compassion requires a personal, human-to-human connection, built on love, understanding and commitment.
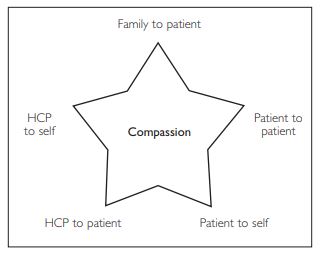
This essay examines the integral role of compassion within healthcare, highlighting five key points of the ‘star’ from which compassion radiates (Figure 1). It draws on my experiences as a patient, a relative and a medical student.
Compassion of family towards patients
Compassion from loved ones can greatly improve patient health outcomes (Reblin and Uchino 2008). My grandfather, aged 85, recently suffered a basal ganglia stroke, resulting in apathy, lethargy and loss of ability to initiate activity. As a family, our concern and desire to help was immediate, but demonstrated in different ways. My aunt focused on practicalities, bringing him necessities, securing his house and arranging care for his dog. She worriedly informed the consultant that he would no longer cope at home. My mother and I spent more time listening, trying to understand my grandfather’s psychological difficulties. Until his stroke, he had been a wholly independent and active man. He was extremely proud of never having had any health problems, not taking any medication and still being able to touch his toes. The stroke robbed him of his confidence; he now doubted his physical and mental capabilities. Although the stroke had caused mild cognitive impairment, his despair and hopelessness were more related to his psychosocial realisations. This is where compassion was so essential in supporting my grandfather’s recovery; it restored his self-belief, gave him hope and showed him that he could still live an independent life. We worked with clinicians to facilitate discharge, then stayed with him to support and encourage him to do as much as possible for himself. Gradually his confidence and mood improved. He is now once again a cheerful, positive, active man.
Compassion between patients
The value of compassion between patients is often unnoticed. Supportive relationships between patients can provide companionship, understanding and hope (Kornhaber et al). Patients can also learn from and motivate each other towards recovery. When I was aged 18, I was hospitalised for anorexia nervosa. Away from my family in an unfamiliar environment, I felt vulnerable and insecure, compelled to confront overwhelming emotional challenges. During our time in hospital, a small group of us grew close, supporting each other through every battle. We became attuned to one another, able to detect the subtle signs of someone struggling and in need of a joke or a hug. When I was low, they reminded me that I was loved and valued. When I did the same for them, it reminded me of my own significance, giving me a sense of purpose and fulfilment from helping someone else. Benjamin Gray likewise describes his experience of ward friendships being valuable for both parties (Gray 2013). However, while controlled support groups may offer a degree of peer support, they do not necessarily generate mutual compassion. Our numerous facilitated ‘group therapy’ sessions on the ward were silent, strained and superficial. Involving the whole ward, they failed to utilise natural friendships which had formed between individuals. They felt forced and, under scrutiny, we were unable to share our feelings. This may partly explain the poor uptake of some peer support programmes (Taylor et al 2015). Compassion between patients can be encouraged, but not compelled.
Compassion of patient to self
Self-compassion for some patients is enormously challenging (Allen and Leary 2010). It means accepting illness and recognising that they are worthy of care. A few years ago, I was diagnosed with an auto-immune type condition; unpredictable flares cause me extreme fatigue, fevers and widespread pain. When first diagnosed, I was determined not to be fazed; my stubborn and pragmatic personality insisted on being resilient. When unwell, I pushed myself into lectures, wearing multiple jumpers to control my shivering and heat packs to comfort the pain. My concentration was poor, and productivity limited, but I was determined not to be ‘weak’. My attitude has since changed considerably. Through working with my psychologist, I have begun to accept my illness and ‘allow’ myself to be unwell. He challenged my unrealistic expectations of myself, showing me that my self-worth should not be determined by my productivity. While it is still difficult and frustrating to force myself to rest when unwell, I now acknowledge that it is necessary and important for my welfare.
Compassion of healthcare professionals to patients
Compassion seems an obvious requirement of healthcare professionals. Following the Stafford Hospital scandal, David Cameron called for nurses to be employed and rewarded based on their demonstration of compassion (Campbell 2013). But ‘compassion’ motivated by reward is surely no longer compassion. Dr Anna Smajdor writes that compassion is ‘not necessary’ in healthcare, since quality care can be delivered without it (Smajdor 2013). However, although compassionless care may effectively treat disease, it does not treat the individual. Holistic care always has compassion at its centre; I have observed many examples of this in clinical practice. In one GP consultation, a middle-aged lady presented with diarrhoea, visibly upset. Her symptoms were not severe and her distress seemed disproportionate. A medically efficient response was to end the consultation briskly, identifying her medication (metformin) as the cause. However, the GP was genuinely concerned about her level of distress so gently probed further. With some embarrassment, she confessed to humiliating incidents of soiling her clothing. By understanding her mortification, the GP was able to offer sympathy and support, promising they would work together to prevent recurrence. The patient then revealed additional fears. It transpired that she had recently cared for her husband through gruelling treatments for bowel cancer, which had also begun with diarrhoea. The GP took time to comfort and reassure the patient, showing her the result of her negative bowel screening test and explaining the gastro-intestinal side effects of metformin. The patient’s relief was tremendous; the whole room suddenly breathed and relaxed. The outcome of the consultation from a medical perspective was identical with or without compassion – a reduced dose of metformin. However the outcomes achieved by the compassionate GP extended much further. This will no doubt enhance the patient’s compliance, psychological wellbeing and future ability to trust physicians.
Compassion of healthcare professional to self
It is not only patients who need to acquire self-compassion. It is acknowledged that physicians (and other HCPs) have a high rate of ‘burn-out’ due to a pressured culture which demands invincibility and self-sacrifice (Nedrow et al 2013). Strategies have been proposed to boost physician resilience, including stress management, supportive relationships and boundaries (Jensen et al 2008; Zwack and Schweitzer 2013). While these may be beneficial, it can be argued that maximum effectiveness will only be achieved through self-compassion. Preserving physician health is frequently justified on the grounds of improved clinical efficiency (Wallace et al 2009). However, protecting our health purely to enhance productivity means we forget that we too are worthy of being well for our own sake, not just for that of other people. A doctor who resentfully goes to the gym to maintain their work capability will benefit far less than a doctor who embraces this time as a well-deserved, satisfying leisure pursuit. I know a GP who keenly protects his leisure time to take part in basketball and squash. He has learnt to prioritise and delegate, and to accept that it is not always possible to complete tasks perfectly. He acknowledges that he deserves time to unwind and the promise of an enjoyable evening keeps him motivated, fulfilled and satisfied.
Conclusion and implications for clinical practice
Patient-centred medicine which retains compassion can improve patient trust, satisfaction, compliance and health (Reynolds 2009; Stewart et al 2000; Epstein et al 2010). We cannot force professionals to display compassion, but we can lead by example, displaying compassion in our own practice. We can involve a patient’s family in their care, inquiring about the patient’s premorbid character and assisting the family to motivate and engage their loved one. On the ward, we can introduce patients to each other, recognising individuals who would appreciate peer support and facilitating patient interactions over mealtimes. We can remind our patients of their intrinsic worth, encouraging them to prioritise their own welfare and educating and empowering them towards self-care. We can take the time to listen, gently exploring patients’ concerns and forming a genuine relationship which recognises their individuality. And finally, we can try to recognise our own innate value by protecting and embracing our own wellbeing. There may not be physical rewards for professionals who demonstrate compassion, but the job satisfaction and personal fulfilment, not to mention the benefits to patients, are immeasurable.
References
- Allen AB, Leary MR (2010) Self-compassion, stress, and coping. Soc Personal Psychol Compass 4(2) pp 107–118
- Campbell D (2015) David Cameron’s prescription for NHS failings: target pay of nurses. The Guardian Online, February 6. Available at: http://www.theguardian.com/society/2013/feb/06/david-cameron-nhsnurses (accessed 2 March 2015).
- Epstein RM, Fiscella K et al (2010) Why the nation needs a policy push on patient-centered health care. Health Aff (Millwood) 29(8) pp 1489–95.
- Gelhaus P (2012) The desired moral attitude of the physician: (II) compassion. Med Health Care Philos 15(4) pp 397–410. Gray B (2013) Peer support in hospital – a shared journey. Schizophr Bull 39 (1) pp 3.
- Jensen PM, Trollope-Kumar K et al (2008) Building physician resilience. Can Fam Physician 54(5) pp 722–9.
- Kornhaber R, Wilson A et al (2015). Inpatient peer support for adult burn survivors-a valuable resource: a phenomenological analysis of the Australian experience. Burns 41(1) pp 110-7.
- Lang R (2007) Paper 3: The development and critique of the social model of disability. Available at http://www.ucl.ac.uk/lcccr/lccstaff/raymond-Lang/developmment_and_critique_of_the_social_ model_of_d.pdf (accessed on 2 March 2015).
- Leget C, Olthuis G (2007) Compassion as a basis for ethics in medical education. J Med Ethics 33(10) pp 617–620.
- Nedrow A, Steckler NA, Hardman J (2013) Physician resilience and burnout: can you make the switch? Fam Pract Manag 20(1) pp 25-30.
- Reblin A, Uchino BN (2008) Social and emotional support and its implication for health. Curr Opin Psychiatry 21(2) pp 201–205.
- Reynolds A (2009) Patient-centered cre. Radiol Technol 81(2) pp 133–47.
- Shakespeare T (2013) A point of view: How important is compassion in healthcare? BBC news, June 7. Available at: http://www.bbc.co.uk/ news/ magazine-22773043 (accessed on 2 March 2015).
- Smajdor A (2013) Reification and compassion in medicine: A tale of two systems. Clinical Ethics 8 pp 111–118.
- Stewart M, Brown JB et al (2000)The impact of patient-centered care on outcomes. J Fam Pract 49(9) pp 796–804.
- Taylor F, Gutteridge R, Willis C (2015) Peer support for CKD patients and carers: overcoming barriers and facilitating access. Health Expect, doi: 10.1111/hex.12348 (Epub ahead of print).
- Wallace JE, Lemaire JB, Ghali WA (2009) Physician wellness: a missing quality indicator. The Lancet 374(9702) pp 1714–1721.
- Zwack J, Schweitzer J (2013) If every fifth physician is affected by burnout, what about the other four? Resilience strategies of experienced physicians. Acad Med 88(3) pp 382–9.






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}