

Five windows on suffering – knowing and celebrating who we are
William House
Published in JHH12.3 – Beyond Peak Medicine?
William House is Chair of the BHMA, GP researcher, and also Chair of an experimental community development organisation. Here William introduces this article and himself, for he is the toddler illustrated with ‘Window 4’, as he prepares for a life as an artist!
Now that I have retired after 30 years in general practice I am trying to understand what I was really doing all that time.This article is some of the fruit from this task: I am being the pathologist to my career. Of course, I tried hard to understand while I was still working as a GP, but some explanations reveal themselves only at the post mortem examination. So now, like all those who dissect the past, I have the last word. But I can do little more than chide or cheer younger hapless clinicians as they struggle with the cut and thrust of real raw life and do or do not make sense of who they are and what they are doing.
When we see things in the world, we rescue them from formlessness by giving them form. Share on X
Window one: medical diagnosis
A few months ago I was at a meeting in the town where I practiced as a GP for 27 years. I was approached by a woman in her 50s who I had got to know in my new role in community development. She reminded me of a time about 25 years ago when I had been in my GP practice for about 10 years. She had rung me late at night about her daughter, Jenny (not her real name) aged seven. I began to remember. I was just getting ready for bed. In those days we five partners shared the 24-hour emergency medical cover for our patients and it was my evening and night on call. The phone rang and I heard an anxious mother. I knew her vaguely but she was not a frequent attender. She was worried about Jenny who was very hot and seemed quite ill. I put on my clothes over my pyjamas and went to see her. She had a high temperature and was listless but quite lucid and I couldn’t find anything else on examination. So I gave my usual advice and went home to bed.
At 6 o’clock the next morning the mother rang again to say she’d got the spots I had told her about, and these were, of course, those of meningococcal septicaemia. I was there in my pyjamas in about 5 minutes and she was in hospital 15 minutes after that – ambulances were very quick in those days and it was before GPs were advised to give a penicillin injection to such patients. I don’t remember hearing the outcome but she wanted to tell me as we stood by the coffee machine at the end of the meeting. Jenny had been very quickly treated at the hospital, and though she developed meningitis she slowly recovered. About two years later she had a grand mal fit and turned out to have epilepsy. Maybe she would have got this anyway, but the mother continued: ‘She was never very good at taking tablets, but we made sure she did and she was OK. But when she left school things started to go wrong for her; she started illicit drugs and stopped taking her prescribed anticonvulsants. One day she was found dead in her room. She was 27 years old. I didn’t know how to respond. Her mother told me this story calmly and there was no sense of blame attached to me. But I asked myself: would this tragic sequence of events happened if I had sent her into hospital the evening before? There is a sense in which medical diagnosis is a tyranny – a mother’s tyranny in this case. I was left profoundly moved by that little conversation, and thought about it a great deal. I first told this story at a British Pain Society conference themed on the ‘Tyranny of Diagnosis’. Though a tyranny to parents, meningococcal disease is well understood through the medical model and (if caught early) can be cured by the technological treatments. But many, perhaps most, illnesses are not like this. Even most infective illnesses have other factors which are at least equally important and must not be ignored. My purpose with the story was to set a context in which to examine another sort of diagnostic tyranny which wears down many of us in a different way: the tyranny of overdiagnosis: extending ‘diagnosis’ beyond its usefulness.
septicaemia. I was there in my pyjamas in about 5 minutes and she was in hospital 15 minutes after that – ambulances were very quick in those days and it was before GPs were advised to give a penicillin injection to such patients. I don’t remember hearing the outcome but she wanted to tell me as we stood by the coffee machine at the end of the meeting. Jenny had been very quickly treated at the hospital, and though she developed meningitis she slowly recovered. About two years later she had a grand mal fit and turned out to have epilepsy. Maybe she would have got this anyway, but the mother continued: ‘She was never very good at taking tablets, but we made sure she did and she was OK. But when she left school things started to go wrong for her; she started illicit drugs and stopped taking her prescribed anticonvulsants. One day she was found dead in her room. She was 27 years old. I didn’t know how to respond. Her mother told me this story calmly and there was no sense of blame attached to me. But I asked myself: would this tragic sequence of events happened if I had sent her into hospital the evening before? There is a sense in which medical diagnosis is a tyranny – a mother’s tyranny in this case. I was left profoundly moved by that little conversation, and thought about it a great deal. I first told this story at a British Pain Society conference themed on the ‘Tyranny of Diagnosis’. Though a tyranny to parents, meningococcal disease is well understood through the medical model and (if caught early) can be cured by the technological treatments. But many, perhaps most, illnesses are not like this. Even most infective illnesses have other factors which are at least equally important and must not be ignored. My purpose with the story was to set a context in which to examine another sort of diagnostic tyranny which wears down many of us in a different way: the tyranny of overdiagnosis: extending ‘diagnosis’ beyond its usefulness.
There is a growing global movement against the overuse of diagnosis – effectively the medicalisation of society and of ordinary human travails adding to the unsustainability of the NHS. The movement, known as ‘Preventing Overdiagnosis’ or POD, is very exciting for us in the BHMA. Though it is not itself a window on suffering, it provides a space in which to introduce holistic understandings of suffering. But POD is a fledgling rebellion and diagnosis remains a powerful and dominant force.
Preventing overdiagnosis: strand 1
There are three strands within the POD movement. The first focuses on medicalising well people by screening for biochemical or radiological indicators of possible disease at a future date – or ‘pre-disease’. This leads to the creation of numerous new ‘diagnoses’ which legitimise further investigations, the prescription of pharmaceuticals, such as statins, and other sometimes invasive treatments for well people. There has been a vast increase in the number of officially recognised diagnoses and of expensive and potentially harmful treatments. Many of them are more beneficial to healthcare providers than to patients.
Preventing overdiagnosis: strand 2
The second strand within POD is to question the dominant role of evidence-based medicine or EBM, started as an attempt to ensure that the NHS in the UK uses only treatments that work. The EBM rationale is heavily dependent on diagnosis as a marker of illness and science in the evaluation of what works. Many now say that EBM has squeezed out subtler forms of understanding illness and wellness – that it has become ‘evidence dictated medicine’. Powerful academic and commercial institutions with their own agendas have great influence over the generation and dispersal of scientific evidence. Practicing clinicians are deluged with protocols and guidelines devised by expert committees and, in primary care, linked explicitly to performance-related pay. Most fundamentally, this diverts the clinician’s attention away from the human being – both patient and practitioner – adding a lack of humanity to the overuse of diagnosis as an explanation of suffering.
Preventing overdiagnosis: strand 3
By the time I qualified as a GP in 1979 – nine years after leaving university – I was already very interested in the more mysterious aspects of suffering. I could see that medical diagnosis worked much better for some illnesses than others. Not deterred, the profession has persisted with trying to shoehorn patients labelled with irritable bowel syndrome, chronic pelvic pain, chronic fatigue, fibromyalgia and many more into the medical model of pathogenesis. These labels do little to help the sufferer. Some call them ‘mind-body illnesses’ evoking the problem with relationship that is often at their core. But this term has been very slow to catch on. More popular is ‘medically unexplained physical symptoms’ or MUPS. In September 2014 the second international conference on Preventing Overdiagnosis was held at Oxford University. The BHMA held a workshop with the title, ‘If we are diagnosing too much what are the alternatives?’ We asked the participants, GPs and consultants from all over the world, to bring stories about real patients for whom making a diagnosis was not helpful. We divided them into groups to share their stories and asked them to try to work out why diagnosis was not helpful and then what might help. We were struck most by the lack of ideas – the frustration that they did not know what else to do.
Window two: labels
I have already mentioned that some diagnoses are no more than a label, but this does not make labels useless. Paddington Bear’s label famously reading ‘Please look after this bear’ was valuable to him in Michael Bond’s celebrated stories. Perhaps it was Paddington’s vulnerability, as much as his label, that endeared him to so many readers. Though we may not quite wear such an explicit label around our necks, the image of ourselves that we display to the world has a big impact on how we cope, whether we become ill and how we can thrive again.Maria Bello is an American lesbian icon. She talks a lot about labels. One of her memorable quotes is ‘Figure out which labels disempower you and which labels shine with the light of the beauty of who you are or are meant to be’. In the story with which I started this article, Jenny acquired the label ‘I am an epileptic’. What impact that had on what subsequently happened I do not know but it made me think a lot about labels.
In 2006 I became a GP commissioner. As part of our preparation, the practice based commissioning executive, of which I was a part, were encouraged to undertake the Belbin team role inventory, based on Jungian personality types. I learnt that I was a ‘plant’. This means that I am ‘individualistic, serious-minded and unorthodox’. Plants may also have ‘genius, imagination, intellect and knowledge … and be impatient with and disregard practical details and protocols’. This description fitted me like a glove, though while many geniuses may be plants, not every plant is a genius! Nevertheless, this label enabled me to make sense of the way I am, and I felt empowered by it. However, though I frequently pitch up at Paddington Station, I don’t wear a luggage label round my neck. Not yet anyway! Then recently a friend called me a ‘tempered radical’: described by Meyerson and Scully (1995) as ‘individuals who identify with and are committed to their organisation and also to a cause, community or ideology that is fundamentally different from … the dominant culture of their organisation. Their radicalism stimulates them to challenge the status quo. Their temperedness reflects … what they see as injustices or ineffectiveness, and are inclined to seek moderation….’ So, being tempered, I would always stop short of causing serious trouble. My strategy has been tell whoever will listen what was crazy about the way things are, but in the end, to knuckle down and get on with working the system as it is. So this was another label to add to my collection that helped me to cope with life. It is interesting that both of these labels were given to me by others and they helped me to understand and accept, perhaps celebrate who I am. This is a key part of self knowledge. The label must be one that helps us to flourish as a person. Then we are not only healthy in ourselves but acquire another way of helping others who have lost their way in the world. As a practitioner we may slip from scientist to diagnostician, priest, vulnerable friend…. as the situation demands. I am sure this can be helpful but only if there is an underlying authenticity. The label or identity we adopt must be about recognising our own nature, not part of idol worship, of admiring someone you would like to be like but who is actually very different.
Window three: psychological flexibility
In December 2009 an international conference in the Netherlands took a fresh look at the definition of Health (BMJ 2011). It was suggested that health should be understood as ‘the ability to adapt and to self manage’. This is a big change. It is about action, not structure: the key words, ‘to adapt’, ‘to self manage’ are verbs, not nouns. They depict health as dynamic and fluid rather than static and structural. They are positive attributes of health, not the absence of disease. According to this understanding, people with a long-term condition can be as healthy as any other person. In the same way it is possible be feel ill, and yet be healthy. Disease and illness are not opposites of health, they are on different planes of experience. This sort of health is not the exclusive province of experts and is naturally sustainable.
Using the term ‘psychological flexibility’ research psychologists have developed an understanding of health that corresponds closely with the meaning that emerged from the Netherlands conference. The corollary, psychological inflexibility, is believed to be at the root of many behavioural and physical health problems. The psychological literature relevant to this is difficult for the non-specialist but it relates to certain fixed ideas and behaviours based on past experiences and held in the form of words:
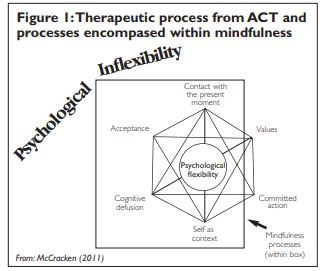
‘The notion is that people often experience the world from inside verbal constructions of the world, including constructions of the past, the future, or the self. Behaviour patterns that emerge from these verbally based experiences are simply less flexible…. When behaviour is dominated by verbally based experience and under the influence of processes we might call ‘inside the head,’ it can be inconsistent with what the environment affords in relation to values or goals’ (McCracken 2011). A therapy called acceptance and commitment therapy (ACT), has emerged from this research and has been
successful in some forms of mental illness and in severe chronic pain. Behind the difficult language is a set of ideas that combines Buddhist teachings with a holistic ‘therapeutic stance’. It acknowledges that suffering is ubiquitous but not inevitable; that avoidance of suffering perpetuates it – hence ‘acceptance’ in the name; that commitment is essential and requires attention to the context of the suffering and a process of letting go (see Figure 1 and more in William House’s column in this issue).
Window four: creative art
This is about using some of the processes of creative art to understand suffering in a way that reveals new healing possibilities. Though poems in the waiting room, dance for postnatal depression or bibliotherapy are often very helpful as therapy, they are not windows on suffering in the way I mean it. This ‘window’ is about seeing everyday practice as an art form.
In 2004 I attended a lecture in London by Rita Charon, physician, literary scholar and leader of the US narrative medicine movement. It was a turning point in my life that enabled me to understand that much of what I did as a GP could be understood as creative art – you might call it ‘the art of medicine’. I captured this quote from the lecture (with resonance from the biblical book of Genesis):
Then she drew on French philosopher Paul Ricoeur’s interpretation of the Aristotelian concept of mimesis. This involves a threefold process expressed by Ricoeur as attention: taking notice, looking, listening; representation: in visible and/or audible form; affiliation: sharing the representation with others. This is a creative and imaginative process still pursued by most artists and with obvious resemblance to the medical consultation – history and examination (= attention), establishing an interpretation or understanding (= representation), sharing with patient and perhaps others (= affiliation) (House 2015). While the ‘representation’ is the ‘form’ or the ‘art work’, in a consultation it could range from a few words or a gesture that signifies understanding, to a verbal explanation or a story that will have meaning for the particular patient or a referral for investigation or a specialist.
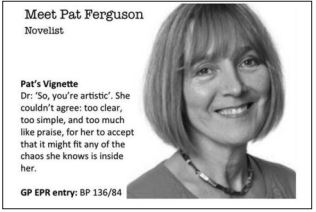 Ten years ago I led a small research project which involved placing a novelist (who had been a nurse and midwife in an earlier life) in 55 GP consultations (with full patient consent) and asking her to write a very brief vignette about each patient. We then shared selected vignettes with the GPs in Focus Groups. Some of the writings triggered startling revelations, including one comment that provided the title for the later publication: ‘We are not human beings in medicine any more’ (House 2012). Many of these ‘representations’ were rich with meaning. An example is given with the picture.
Ten years ago I led a small research project which involved placing a novelist (who had been a nurse and midwife in an earlier life) in 55 GP consultations (with full patient consent) and asking her to write a very brief vignette about each patient. We then shared selected vignettes with the GPs in Focus Groups. Some of the writings triggered startling revelations, including one comment that provided the title for the later publication: ‘We are not human beings in medicine any more’ (House 2012). Many of these ‘representations’ were rich with meaning. An example is given with the picture.
Window five: the healer
The picture of the little boy in the Window Four section is me when I was aged three. I grew up in an isolated spot surrounded by nature and art. My father was a painter, my mother sang opera, and my much older sister was a pianist – at least in her youth. I tried quite hard with music on and off, but wasn’t very good. Perhaps I could see that I couldn’t compete with my sister, so despite the pose for the photo, I spent my youth fiddling with machines and being good at science, both of which my sister was hopeless at. But the art never left me. At university I revived the music society and formed an orchestra and a choir along with my talented violinist girlfriend, but I was
still searching for something else. It was not until many years later, after hearing Rita Charon speak, that I realised that much of what I did in the GP surgery was actually being the creative artist I was born to be. I had found my artistic outlet without realising it. Now I understood why I so much enjoyed what I was doing.
There is perhaps something special about vocation, about loving what you do. As I faced the need to say goodbye to my patients at the end of my career, I realised that I felt a kind of love for them. Other doctors have written this too. In her heartfelt 2012 lecture, ‘Love’s
Labours Lost’, Iona Heath talks about the different kinds of love for which the Greeks have four words, whereas in English, we have only one. She suggests ‘agape’ is the best word for the ‘disinterested but unconditional commitment needed by professionals’ (Heath 2012). Whatever we might call it, I believe there can be a quality of connection built up over many years from which a mutual understanding of suffering can emerge and exercise healing qualities. This is really quite ordinary. It is the power of relationship to understand and to heal.
References
- Heath I (2012) Love’s labours lost: why society is straitjacketing its professionals and how we might release them. Available at: http://www.internationalfuturesforum.com/u/cms/Iona_Heath_Lecture2 012.pdf (accessed 16 November 2015)
- House W (2015) Too much diagnosis and not enough art. Journal of Holistic Healthcare 12(1) pp 26–29.
- House W (2012) We are not human beings in medicine any more. Journal of Holistic Healthcare 9(2) pp 38–44.
- Huber M et al (2011) Invitational conference ‘Is health a state or an ability? Towards a dynamic concept of health’, report of the meeting December 10–11. BMJ 343:d4163. McCracken LM (2011) History, context, and new developments in behavioral medicine. Books.google.com
- Meyerson DE, Scully AS (1995) Tempered radicalism and the politics of ambivalence and change. Organization Science 6(5). Available at: http://www2.massgeneral.org/facultydevelopment/owc/pdf/Tempered% 20Radicalism%20and%20the%20Politics%20of%20Ambivalence%20and %20Change.pdf (accessed 17 November 2015).






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}