

A vision for sustainable healthcare
Trevor Thompson, GP; Reader in healthcare education, University of Bristol
Knut Schroeder, GP; Honorary senior clinical lecturer, Centre for Academic Primary Care, University of Bristol
Published in JHH12.1 – Future horizons
With the cliffs and curves of my native Irish landscape etched deep into my soul, I’ve has always had a fascination with the home planet and planned to be a geologist before discovering medicine. Now in mid-career I am delighted to find my love of clinical medicine and ecology converge in sustainable healthcare. My latest passion is a project called Green Impact for Health which rewards GP practices for pro-sustainability actions. My favourite bit of Green Impact is the green prescription – official, physicianly encouragement for people to get active in nature.
Trevor Thompson
My interest in making healthcare more sustainable started when I attended a conference on climate change and health in London in 2008. For the first time it became clear to me that the health sector not only has to deal with the consequences of global environmental change, but that we also contribute to it – in a big way. I’m currently focusing on developing new ways to help people make better decisions about their health: to help improve their care, reduce the strain on the NHS, and save precious resources.
Knut Schroeder
- Redefining value and health
- Why should health services become more sustainable?
- What will sustainable healthcare look and feel like?
Redefining value and health in healthcare
If we accept that the greatest future challenges to global health are climate change and environmental sustainability, what might better birth, healthcare and end of life care look like if we were to model them around resilience and adaptability?
Implicit in any such redefining of health and healthcare is the question of value. When ‘value’ relates to commodities, they are higher priced, rarer and more exclusive – stylish clothes, luxury cars, long-haul flights – and, intriguingly their value is often proportional to their carbon cost, the waste they produce and resources they consume. In contrast, whatever can be sustained (healthcare for example) accentuates values which are not commodifiable, In fact compassion, kindness, caring, fun, friendship, conversation, mindfulness or being in nature – all of which have been shown to have clear health benefits – are potentially limitless.
Why health services must become more sustainable
Health systems can create health problems (for example adverse reactions and patient safety) and contribute to climate change. The World Health Organization’s (WHO) Director of Public Health and Environment, Maria Neira, wrote that ‘Hospitals are energy and resource intensive enterprises that, as they operate today, contribute substantially to climate change while inadvertently contributing to respiratory and other illnesses’ (WHO 2009). In Health Care Without Harm WHO emphasises the role of health services in reducing the magnitude and consequences of climate change.
The ecological impact of healthcare delivery would be one element in a holistic and sustainable system of prevention, cure and care. Healthcare providers need considerable amounts of energy and resources to provide clinical care and operate smoothly. Supplying medicines, procuring food and goods for patient care and using resources like natural gas for heating and petrol for transporting patients all carry a substantial carbon footprint (see case study 1).
Case study 1 Health systems and carbon emissions: example statistics
- In 2007, the US healthcare sector accounted for 16% of US gross domestic product and was responsible for eight per cent of total US greenhouse gas emissions (US Department of Energy 2009).
- In the UK, the NHS calculated that its annual carbon emissions in 2007 was more than 21 million tonnes of CO2e, which is about a quarter of all emissions from the public sector in the UK (NHS 2008). Broken down, procurement topped the list of individual contributions with 60%, followed by building energy (22%) and travel (18%).
- According to the US Department of Energy, US hospitals use 836 trillion British thermal units (BTUs) of energy at a cost of US$ 5 billion (£3.2 billion) every year, which is more than double the energy use and carbon emissions of all standard US office buildings (DoE 2011).
- In Brazil, hospitals consume an estimated 10% of the total commercial energy.
Although calculating the exact carbon footprint of any health service around the world is impossible, the estimates suggest that it is very large indeed. By reducing carbon emissions and making better use of resources, health systems could contribute to mitigating climate change, improving population health while doing so.
Addressing inefficiencies in health provision
Inefficiencies are common in the health sector, even in technologically and economically advanced countries. For example, the US health system has been described as inefficient not only because of high administrative costs, fragmented care, and differences in the quality of treatment for patients depending on users’ race, income and where they live. Though there is no ‘perfect’ health service, improvement is always possible by using resources responsibly and working more effectively to reduce carbon footprints, make financial savings, improve compliance with legislation, increase resilience and, most importantly, improve quality of care.
Responding to national frameworks, targets and international initiatives
Healthcare institutions have good reason for trying to be ahead of the game. Moreover, organisations in the UK are legally required to reduce their greenhouse gas emissions by 80% by 2050 compared with levels in 1990 under the Climate Change Act 2008. The US has committed to reducing its emissions to 17% below 2005 levels by 2020 (World Resources Institute 2015). The EU has committed to cutting its emissions to 20% below 1990 levels by 2020 (European Commission 2015). Similar regulations apply in many other countries.
Case study 2 Implementing sustainable development at international level
A number of countries have developed strategies to implement sustainable development.The Division of Sustainable Development (DSD) of the UN Department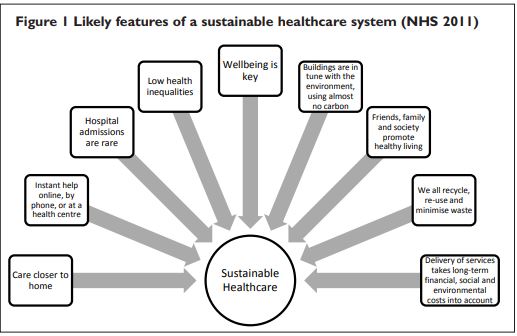 of Economic and Social Affairs provides leadership and expertise at international level within the United Nations on sustainable development (United Nations 2015).The UK government published its strategy document Securing the Future in 2005, promoting a more sustainable economy, the responsible use of sound science, and good governance (Defra 2005).The priority areas laid out in this document include sustainable consumption and production, climate change and energy, protecting natural resources and the environment, as well as creating sustainable communities in a fairer world. In the US, the Bureau of Oceans and International Environmental and Scientific Affairs of the US Department of State lead a number of partnerships and initiatives that promote economic growth, social development and environmental stewardship.
of Economic and Social Affairs provides leadership and expertise at international level within the United Nations on sustainable development (United Nations 2015).The UK government published its strategy document Securing the Future in 2005, promoting a more sustainable economy, the responsible use of sound science, and good governance (Defra 2005).The priority areas laid out in this document include sustainable consumption and production, climate change and energy, protecting natural resources and the environment, as well as creating sustainable communities in a fairer world. In the US, the Bureau of Oceans and International Environmental and Scientific Affairs of the US Department of State lead a number of partnerships and initiatives that promote economic growth, social development and environmental stewardship.
Healthcare institutions have good reason for trying to be ahead of the game. In 2009, The Lancet published a landmark series of papers illustrating the sometimes striking short-term health benefits to be gained from actions to tackle climate change (Horton 2009, Chan 2009, Gill and Stott 2009, Haines et al 2010). Sustainable healthcare will need to live and work within our means with regard to natural resources. It would not endanger current and future population by putting detrimental stress on local or global environmental and human systems.
The UK NHS Sustainable Development Unit has outlined some characteristics of a sustainable healthcare system by creating a picture (Figure 1) of how the NHS could address needs today without prejudicing our ability to do the same in future (NHS 2011).
This depicts a system where everyone does their best to provide the best quality of care, while promoting healthy living and minimising human impact on the environment. The scale of the challenge is huge but so too is the scale of the opportunities, for they demand far more than just delivering efficiencies. In fact we need entirely to re-examine our rationale for maintaining health and addressing illness, and completely re-evaluate the economics of healthcare.
Components of a more sustainable and holistic health sector
Although the future shape of the NHS is far from certain, Forum for the Future and the UK National Health Service Sustainable Development Unit have developed scenarios for less carbon dependent and resource-aware services. Case study 3 gives some examples (NHS SDU 2009a).
Case study 3 Possible features of more sustainable societies (adapted from Fit for the Future)
- The high price of carbon has created a new type of consumerist world where businesses sell services (for example, wellness-coaching) rather than products (such as pharmaceuticals), and where good citizens share more with their neighbours
- Communities work together to support healthy lifestyles and businesses take increasing responsibility for promoting public health.
- Countries prioritise economic and social resilience over growth, and quality of life is the key goal.
- People value meaningful work, low-impact lifestyles and their community.
- Healthy living is a high priority, and much care is delivered through friends, families and charities.
- Workplace health schemes are common.
- Rapid innovation and novel technologies have created a low-carbon economy.
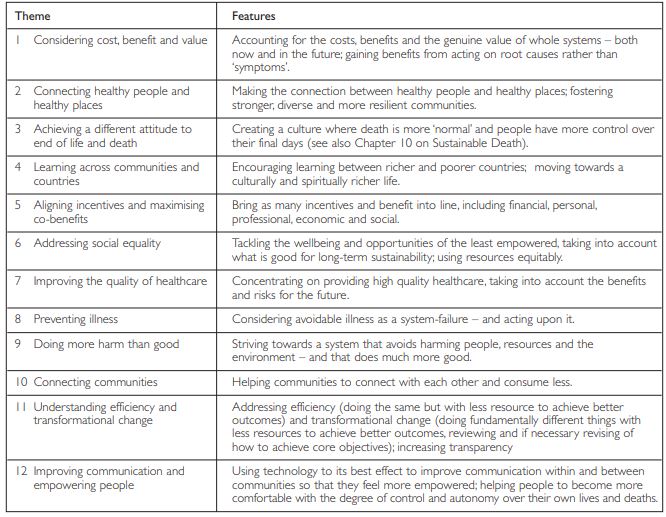
12 themes are likely to determine a sustainable and low carbon health system (Pencheon 2011).
Models of care
Sustainable health systems can only be viable within sustainable communities that invest and engage in preventive care by better integration of health services with other sectors: for instance community networks, housing/planning/transport departments and educational organisations. Consider for instance the provision of energy efficient housing for vulnerable people, or working with local authorities to encourage active travel by prioritising investment in cycle paths that make it easier to choose walking, cycling or public transport over car use. Both strategies would contribute to people’s health and life quality while also saving energy and money.
Drivers of change include shifting demography, new technologies, changing expectations (clinicians’ as well the public’s), resource limitation, globalisation as well as environmental and climate change. Future hospitals may be very different places emphasising health more than disease. They could be smaller, more targeted to the needs of a more local community. Many hospital services might even become redundant in some respects as more care is provided in the community and in people’s homes.
Sustainability governance in healthcare
Healthcare in the future may also be less hierarchical, with more skill- and task-sharing by professionals for whom sustainability is as important as high quality of care. Healthcare managers will take environmental and social responsibilities as seriously as financial governance, reporting in all three areas through an approved Board and reviewed regularly against its agreed Sustainable Development Management Plan (SDMP). Various organisations such as Healthcare Without Harm, the Climate and Health Council, Swedish Doctors for the Environment or Doctors for the Environment Australia are already encouraging health professionals to lead by example and take up the cause of sustainable development.
The co-benefits of sustainability actions
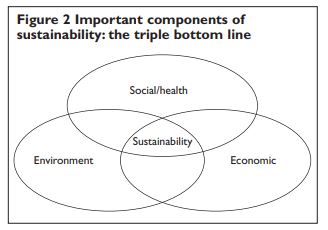 Fortunately, reducing carbon footprints and making better use of resources could create opportunities for substantial savings. Public sector healthcare will always face financial constraints, yet though this might seem an obstacle to change, this reality actually supports the case for making health services more sustainable, because considering sustainability in all that they do would allow healthcare organisations in the longer term to reap significant environmental, health, social and economic rewards. This synergistic triple bottom line of benefits to people, planet, profit (see Figure 2) makes the need for an environmentally friendly health sector even more compelling.
Fortunately, reducing carbon footprints and making better use of resources could create opportunities for substantial savings. Public sector healthcare will always face financial constraints, yet though this might seem an obstacle to change, this reality actually supports the case for making health services more sustainable, because considering sustainability in all that they do would allow healthcare organisations in the longer term to reap significant environmental, health, social and economic rewards. This synergistic triple bottom line of benefits to people, planet, profit (see Figure 2) makes the need for an environmentally friendly health sector even more compelling.
Potential gains from energy savings
As prices of fossil fuels will rise healthcare providers already struggling to meet their energy demands because of limited resources will have to reduce dependence on fossil fuels. This trend will be particularly relevant to large urban hospitals (where hikes in fuel prices and supplies will have greater consequences because of the amounts of fuel used) and remote clinics, reliant on long distance deliveries. (see Case study 5 and Case study 6).
Case study 4 Example of hospital energy costs in the US
Estimates from the Practice Greenhealth Energy Impact Calculator (EIC) indicate that a typical 200-bed hospital in coal-powered areas in the US Midwest uses about seven million kWh a year. Consequently, such a hospital is responsible for over US $1 million (£629,000) per year in negative societal public health impacts, and US $107,000 (£67,000) a year in direct health care costs.Although such figures can only be estimates, there is little doubt that positive health impacts are likely to be substantial where health services manage to improve their energy efficiency and change to more environmentally friendly sources of energy.
Case study 5 Optimised energy management in India
One of the largest and oldest hospitals in South-East Asia, the Sir Jamshedji Jeejeebhoy (Sir J.J.) Hospital in Mumbai, India, achieved a reduction in energy costs through better energy management. Being a busy and modern hospital that operates 24 hours a day, energy bills – not surprisingly – run high.The hospital’s operating theatres, top-end medical equipment, lighting, high-voltage alternating current systems, water heaters, elevators and water pumps contribute to more than 75% of the total energy bill. In 2001, the hospital authorities took action on a prime ministerial call to conserve energy by aiming to raise awareness about inefficient energy use.The campaign, which used posters, slogans and other measures, was a striking success. By systematically switching off office equipment, repairing leaks in the air conditioning and making better use of natural daylight, the hospital saved 812,000 kWh of electricity between 2002 and 2004.This reduced the hospital’s energy bill by an impressive US$90,000 (£58,000), an amount that could pay for around 475 cataract operations in India assuming a cost of about 10,000 Rs (£122 or US $188) each, thus freeing resources for improving patient care and other activities.
Energy bills – and so carbon emissions – can be equally high for healthcare providers in Europe and North America, where making better use of the available energy creates fascinating stories, too.
Case study 6 Improved energy efficiency in the UK
For the managers and clinicians at the Renal Unit at the Royal Cornwall Hospital, UK, sustainability actions proved a great success – environmentally, financially and clinically. By identifying ways to improve efficiency and change the way they provide care, they set out to reduce their carbon footprint.The results were staggering. By the end of the first year, they achieved carbon reductions of around 33 tonnes of CO2 per year – roughly the equivalent to around 66 return flights from London to Madrid. But not only that – at the same time they also improved the patient experience with about 50 per cent less waiting, reduced journeys and more self-care.The benefits of their actions did not stop here: staff had more time to look after patients, healthcare acquired infections were reduced, and the unit achieved cost savings of £1,200 (US $2,000) per employee per year.After two years, additional actions reduced CO2 emissions by 53 tonnes. Simeon Edwards, Unit Manager, must have been delighted when he reportedly said: ‘We now have cost avoidances running at over £57,000 (US $91,000) a year as a result of this carbon reduction programme. It would be wonderful if we could re-invest some of that into more carbon reductions.
These are not isolated examples: many carbon- and energy-reducing schemes around the world have shown that substantial amounts of money can be saved and so re-diverted to patient care and other priorities.
The benefits of better food management
When healthcare providers such as hospitals move towards a more plant-based diet for their patients and staff and reduce meat and dairy products in the meals they serve they are likely to contribute to reducing methane levels (an important greenhouse gas) from farming. In addition to being more environmentally friendly, a more plant-based diet has less saturated fat, with obvious direct health benefits. Fresh locally produced seasonal products take less energy to produce, particularly because of reduction in ‘food miles’ – and are better for people’s health. Health practitioners by advocating a more plant-based diet to their patients produce smaller scale but similar co-benefits.
Co-benefits from active travel
Moving staff and patients around in buses or cars usually involves carbon-intensive transport. More active travel helps lower risks of heart disease, obesity, diabetes, mild mental illness – and also helps reduce road traffic crashes. Cycling is energy efficient and increase travel-range about 10-times compared to walking. Cycling is cheap, incurs no fuel costs, and far less maintenance than for cars. So encouraging health professionals and patients (those who are able to) to travel more actively is a good starting point.
Active and low-carbon travel also helps improve air quality. The WHO estimates that exposure to fine particulates contributes to about 100 000 deaths and 725,000 years of life lost each year in Europe. Consequently, reducing the environmental impact of carbon-intensive travel in the healthcare sector should be a priority for the healthcare community, particularly in heavily polluted areas.
Monitoring and reducing carbon emissions
Only when the right metrics are available to monitor and review carbon emissions, will healthcare organisations be able to include their true costs in business decisions. Right now though, well-researched metrics for these direct and indirect health impacts are still lacking. Yet there is progress, and the UK National Health Service Sustainable Development Unit and Sustainable Development Commission are preparing a report on the use of carbon metrics for inclusion in regulatory frameworks (NHS SDU 2015).
Case study 7 Measuring carbon emissions
The UK West Midlands Cancer Intelligence Unit demonstrates the importance of measuring carbon emissions.This healthcare organisation has pioneered the use of data from its cancer registry along with a Geographical Information System (GIS) to work out the carbon emissions related to treating breast cancer (NHS SDU 2009b). Figures from 1999 to 2004 indicated a 214% increase in total car miles travelled which equates to over 400 tons of carbon emissions from radiotherapy treatment in the West Midlands. Reflecting on patient and visitor mileage, and therefore carbon emissions, is therefore a useful tool for helping to design lower carbon pathways.
Being accountable for sustainability should become an integral part of good clinical and organisational governance, with every healthcare organisation signed up to an approved sustainable development plan identifying measurable carbon reduction milestones in line with national and international targets. For the UK this would mean a reduction in carbon emissions by 10% of the 2007 levels by 2015, as a minimum.
Using technology to its best effect
Making best use of technology is an important part of sustainable development. Health services can play a vital role in helping to develop and implement lower carbon technologies, which ideally includes support with funding and providing testing grounds for demonstration projects. Information and communication technology (ICT), renewable energy and low-carbon ways of transporting people and goods are example areas where the health sector can be influential in implementing, evaluating and spreading best practice about innovations that not only advance sustainable development, but also deliver better quality of care. Working closely together with academic institutions as well as organisations that specialise in innovation (which may include both the public and commercial sector) will be paramount.
Working in partnership
Yet another synergistic effect of sustainable development is that it drives a process of integration. Health services will by necessity strengthen links with other partner organisations, charities, local businesses, universities and local authorities. This will depend on improved exchange of information and better care pathways, and provide leverage in business planning and new contracts that contribute to sustainable development. This process will embrace the areas so far discussed: purchasing of services and goods, optimal use of renewable energy sources, and more sustainable public and active transport for patients and staff. More ethical and sustainable relationships with pharmaceutical companies will be important too, particularly with pharmaceutical companies providing services for preventing illness rather drugs to treat it.
Case study 8Working with the commercial sector
An example where partnership between the health and private sector can work is the Chesterfield Royal NHS Foundation Trust in the UK.This health organisation teamed up with a commercial firm and entered into a window replacement and ventilation programme that has cut the Trust’s carbon emissions by more than 50 tonnes a year (NHS SDU 2009).
Alternative ways of financing healthcare
Rewarding healthcare providers for activity tends to encourage unnecessary investigations and treatment. To stimulate sustainable health and healthcare we need to align money more towards population needs and outcomes and far less to individuals and activity. Giving large healthcare providers population- and outcome[1]related budgets would incentivise them to align their health, financial and environmental outcomes. This triple bottom line approach would reduce wastage of resources and unnecessary and sometimes harmful healthcare, improve health outcomes, contain costs and induce them to strengthen primary care and prevention. More sustainable business models of healthcare in Spain, India and the USA can sometimes empower patients to take more control of their care through engagement, partnership and information sharing, especially when care is delivered closer to home rather than the more depersonalising milieu of a large hospital (WHO 2015).
Efficiency at the start of sustainable practice
When transforming healthcare systems, change tends to be easier and longer-lasting if driven by staff themselves. A continuous improvement culture empowers staff to make positive changes in the way they work, and this can lead to real benefits in waste and staff morale. The NHS Institute for Innovation and Improvement has pioneered ways of achieving this in secondary care, and in primary care and community settings models such as ‘lean’ technology (NHS Institute for Innovation and Improvement 2015) have been adapted from industry.
Sustainable development is a necessary response to the stresses on individuals, health services and the global community. But in reality the changes called for may not be immediately appealing. This is particularly so where we have been used to certain habits of living and working: air travel is an obvious example. Difficult as it may be we must either inspire and collaborate to tackle these challenges, or face the prospect of fierce or even violent competition further down the line.
Sustainability issues are so closely linked to health, that it seems right for the healthcare sector to set a good example. For inevitably, in the coming decades health and healthcare services will face ecological crises, and to mitigate them and adapt to the problems ahead we must grasp the principles of sustainability and weave them into a vision for sustainable healthcare. Utopian though this vision might seem, many successful initiatives have already been implemented and are under way. Undeniably though, much more needs to be done if we are to have a truly lower-carbon healthcare system in 30 years time. To achieve this everyone working in or with the healthcare sector will have to wake up to the challenge and engage with it. If we can do this, then rather than being traumatic and unexpected, the process of transitioning towards a sustainable healthcare system can be a measured and active one.
Key points
- Healthcare is part of the problem as well as the solution with regard to global environmental change
- Plenty of reasons exist why the healthcare community needs to engage in sustainability, including legally binding frameworks, co-benefits, and current inefficiencies
- The health professions should lead by example
- Key to sustainable healthcare is to make healthcare more efficient
- Sustainable healthcare is low-carbon, supports self-care, makes better use of information and communication technology, and focuses on illness prevention rather than treatment.
References
- Chan M (2009) Cutting carbon, improving health. The Lancet 374 (9705) pp1870–1.
- US Department of Energy (2009) Department of energy announces the launch of the hospital energy alliance to increase energy efficiency in the healthcare sector [internet]. Available at: http://energy.gov/ articles/department-energy-announces-launch-hospital-energy-alliance[1]increase-energy-efficiency (accessed on 12 February 2015).
- DEFRA (2005)The UK Government Sustainable Development Strategy. Cm6467. Available at: http://www.defra.gov.uk/publications/files/ pb10589-securing-the-future-050307.pdf (accessed on 12 February 2015).
- European Commission (2015) EU greenhouse gas emissions and targets [internet]. Available at: http://ec.europa.eu/clima/policies/ g-gas/index_en.htm (accessed on 12 February 2015).
- Gill M, Stott R (2009) Health professionals must act to tackle climate change. The Lancet 374(9706) pp1953–5.
- Haines A, Wilkinson P, Tonne C, Roberts I (2010) Aligning climate change and public health policies. The Lancet 374(9707) pp2035–8.
- Horton R (2009) The climate dividend. The Lancet 374(9705) pp 1869–70.
- NHS (2008) NHS Carbon emissions carbon footprinting report. Available at: http://www.sd-commission.org.uk/data/files/publications/ NHS_Carbon_Emissions_modelling1.pdf (accessed on 12 February 2015).
- NHS Institute for Innovation and Improvement (2008) The productive series. Available at: http://www.institute.nhs.uk/quality_and_value/ productivity_series/the_productive_series.html (accessed on 12 February 2015).
- NHS Sustainable Development Unit (2015) [internet]. Available at: http://www.sduhealth.org.uk/resources/default.aspx?q=carbon+ reduction+strategy (accessed on 12 February 2015).
- NHS Sustainable Development Unit (2011). Route map for sustainable health. Cambridge: NHS Sustainable Development Unit.
- NHS Sustainable Development Unit (2009a). Fit for the future: Scenarios for low-carbon healthcare 2030. Available at: www.sduhealth.org.uk/resources/default.aspx?q=fit+for+the+future (accessed on 12 February 2015).
- NHS Sustainable Development Unit (2009b). Saving carbon, improving health: Carbon reduction strategy for England. Cambridge: NHS Sustainable Development Unit.
- Pencheon D (2011) Towards a lower carbon health system. Journal of Holistic Healthcare 8(2) pp 15–8.
- World Health Organization and Healthcare Without Harm (2009) Healthy hospitals, healthy planet, healthy people: Addressing climate change in healthcare settings. Available at: http://www.who.int/ globalchange/publications/healthcare_settings/en/index.html (accessed on 12 February 2015).
- World Resources Institute (2015) U.S.Climate initiative [internet]. Available at: http://www.wri.org/our-work/project/us-climate-initiative (accessed on 12 February 2015).
- United Nations (2015) Sustainable development knowledge platform [internet]. Available at: http://www.un.org/esa/dsd/dsd/dsd_index.shtml (accessed on 12 February 2015).






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}