

Embodied breathing habits
Aligning breathing mechanics with respiratory chemistry
Peter M Litchfield, President, Professional School of Behavioral Health Sciences
Sandra Reamer, Director of Education, Professional School of Behavioral Health Sciences
Published in JHH 19.2- Embodiment and bodywork
Introduction
Breathing and its potential effects on our lives, positive and negative, are enormous. Appreciating this enormity is significantly enhanced by learning about the amazing physiology of breathing, which together with understanding breathing as motivated behavior, can account for the profound and far-reaching effects of breathing on health and performance (Litchfield, 2006, 2010, 2017).
Millions of people from around the world include breathing learning interventions in one way or another in their professional and/or personal lives for a multitude of reasons, for example relaxation. Most of them, however, focus exclusively on mechanics of breathing (external respiration), for example slow breathing, without understanding and addressing their profound impact on the chemistry of respiration (internal respiration), for example acid-base regulation (pH) of extracellular fluids (eg blood plasma).
Understanding the regulation of this chemistry helps to:
- avoid misguided breathing interventions that can have adverse effects
- avoid faulty conclusions about the nature of breathing interventions and their outcomes
- identify dysfunctional breathing habits that can seriously compromise respiration and precipitate myriad symptoms and deficits
- teach and learn breathing habits that optimize respiration, that is, align breathing mechanics with respiratory requirements
- expand the scope and effectiveness of breathing interventions for personal use as well as for practitioners consulting with clients and patients.
The effects of compromised respiratory chemistry, brought on by breathing habits that misalign mechanics with chemistry, can be immediate and disturbing. Statistics suggest that millions of people worldwide suffer with the profound and misunderstood symptoms and deficits brought on by overbreathing, that is, breathing habits that lead to hypocapnia (CO2 deficit). Surveys suggest that 60% of ambulance runs in the major USA cities are a result of acute symptoms brought on by hypocapnia (Fried, 1999). Unfortunately, these kinds of dysfunctional habits are rarely identified by healthcare practitioners, their effects mistakenly attributed to other causes, and their resolutions prescriptive in nature where focus is on symptoms rather than on causes, for example drug prescriptions.
Breathing behavior analysis can provide a solution to this challenge where dysfunctional breathing habits, ie learned physiological reconfigurations, are identified including their effects, triggers, behavioral components, motivation, reinforcement (outcomes that sustains them), and etiology. Precisely the same principles by which people learn these habits can also be implemented for overcoming these same habits and/or learning new breathing habits that enhance health, learning, performance, awareness, creativity, and communication. Learning about how mechanics and chemistry work together is fundamental to understanding the effects of both unconscious breathing habits and intentional breathing training protocols on health and performance, such as effects on cerebral blood flow. This article provides a brief overview of these considerations, while introducing some basic respiratory physiology relevant to improving the effectiveness of both personal and professional breathing learning applications and interventions.
Breathing and respiration
Breathing and respiration are not the same. Respiration is a subset of breathing. Besides providing for respiration, breathing serves us in many and diverse ways, eg speech. Thinking of breathing as behavior forever changes the way we understand it. The notion of ‘breathing habits’ emerges and with it an accounting of how breathing mechanics can become disconnected from respiratory reflexes, resulting in compromised health and performance.
Respiration can be subdivided into three phases: external, internal, and cellular. External respiration is about breathing mechanics, moving air in and out of the lungs, eg slow/fast, deep/shallow, mouth/nose, diaphragmatic/chest, and more. Internal respiration is about oxygen transport and distribution to tissues, carbon dioxide management, and acid-base regulation (pH and electrolyte balance) of extracellular body fluids (eg blood plasma). Cellular respiration is about creating adenosine triphosphate molecules (ATP) in the mitochondria of cells, which are then subsequently broken down by cells for energy. Carbon dioxide generated during cellular respiration is a precious gas that ultimately makes possible precision moment-to-moment acid-base regulation.
Breathing is behavior. It serves us in powerful and unsuspecting ways. Breathing habits, good and bad, are learned unconsciously and sometimes consciously, for self-regulating emotions, cognitions, personality, coping styles, physiology, health, performance, and consciousness. Breathing is psychological in the sense that experience sets the stage for its reconfiguration. Embedded in this psycho-physiological reconfiguration is a personal history that regulates breathing based on the principles of learning, perception, motivation, reinforcement (benefits), attention, and memory. The richness of the psychology of breathing provides for both its far-reaching benefits and for its, all too frequent, profoundly debilitating effects.
Respiration is reflexive. External respiration is about regulation of breathing mechanics by brainstem reflex chemo-regulatory mechanisms. Although breathing mechanics continuously shift, as a function of being bored or excited, stressed or relaxed, upset or pleased, and meditative or physically challenged, respiration generally remains within an optimal respiratory chemistry envelope. Unless an unconscious habit or intentional manipulation gets in the way, respiratory requirements will dictate the coordination of breathing mechanics in the context of other interacting behaviors such as eating and talking. Compromised respiration during times of challenge is usually a result of learned and specifically triggered breathing habits, not simply a result of fight-flight autonomic nervous system changes.
Respiratory chemistry
Many people believe that good breathing is about moving as much oxygen (O2) as possible into the blood, while simultaneously eliminating (excreting) as much carbon dioxide (CO2) as possible from the blood, through ‘the right’ breathing mechanics. This view is both uninformed and potentially dangerous. Yes, O2 delivery to body cells is essential, of course, but the best way to accomplish this is not so obvious. And yes, excretion of excessive CO2 is critical, but not all of it, only some of it. Contrary to the belief of many, CO2 is a precious body substance and its ever-presence is required not only for health but for life itself.
External respiration (breathing mechanics) is regulated from breath to breath by chemo-regulatory reflexes located in the brainstem (Levitzky, 2007; Khoo, 2011), based on pH, CO2 concentration, and O2 concentration of arterial blood plasma and other extracellular body fluids (not including O2). These reflexes operate through the diaphragm and the external intercostal muscles while at rest. This is one reason if chest breathing predominates, based on having unconsciously learned a breathing habit (where ‘feeling in control’ may take precedence over allowing for the reflexes), that diaphragmatic training can be so fundamentally important, ie clients learn to prefer mechanics consistent with good respiratory chemistry.
Internal respiration plays a key role in acid-base physiology. It regulates the pH of extracellular fluids (arterial blood plasma, lymph, interstitial, and cerebrospinal fluids) by changing the relative proportions of bicarbonate (HCO3-) and carbon dioxide (PCO2) concentrations (eg HCO3-/PaCO2).
Bicarbonate concentration (HCO3-) is regulated by the kidneys and the arterial CO2 concentration by breathing. When either concentration changes, extracellular acidalkali balance (eg in blood plasma) will immediately shift up or down. Breathing can immediately affect pH level, within seconds, positively by the action of reflex mechanisms and positively OR negatively by learned breathing habits.
Brainstem reflexes (external respiration) change breathing mechanics (rate and depth) so as to regulate the pH of extracellular body fluids. However, respiratory chemistry can also be radically influenced by both voluntary self-interventions and unconsciously learned breathing habits comprised of powerful emotional, motivational, cognitive, and other psychological properties. Consequently learned breathing habits can get in the way of these reflexes leading to insidious, outcomes that are typically unidentified and misunderstood by both practitioners and their clients. The predominate behavioral outcome is overbreathing, breathing that results in hypocapnia (CO2 deficit) and respiratory alkalosis (pH higher than 7.45). Hypocapnia can result in profound physiological changes that manifest as a wide range of symptoms and deficits, both short term and long term, which are all too often ‘medically unexplained’. Hypercapnia (excessive CO2) – chemically the opposite ie respiratory acidosis (pH lower than 7.35) – is uncommon.
‘Contrary to the belief of many, CO2 is a precious body substance and its ever presence is required not only for health but for life itself.’
Brainstem reflex mechanisms regulate breathing mechanics (external respiration) such that the correct CO2 concentration is maintained in the alveoli of the lungs (where gas exchange takes place). This ensures that blood moving through the pulmonary capillary network returns to systemic circulation with a CO2 concentration that keeps pH within normal limits. Thus, when one intentionally over-ventilates by taking large breaths, slow or fast, diaphragmatically or in the chest, or through the nose or the mouth, PaCO2 concentration can drop and drive pH upward toward respiratory alkalosis. Simultaneously, the CO2 concentration drops in red blood cells with a subsequent rise in the pH of its cytosol, resulting in unfriendly stingy hemoglobin (Bohr Effect, Levitzky 2007) that more sparingly delivers it oxygen and nitric oxide (NO, a potent vasodilator) to the blood plasma. These combined changes, plasma and red blood cell alkalosis, lead to reduced oxygen and glucose supply to tissues in need, especially the brain and heart.
Compromised respiration
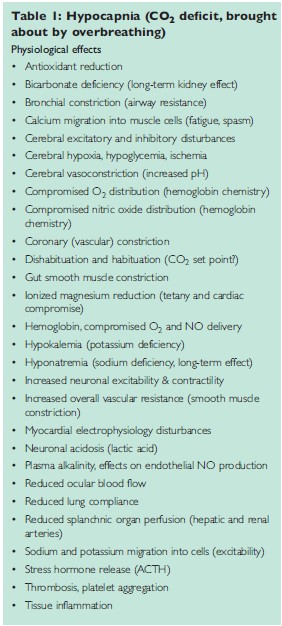
Taking charge of breathing triggered by an unconsciously learned breathing habit, or brought on by a misguided conscious breathing intervention, can easily result in overbreathing (hypocapnia) and its associated physiological consequences: immediate, long term, and widespread (Fried, 1987, 1993; Laffey & Kavanagh, 2002; Maramattom & Wijdicks, 2007), many of which are listed in Table 1 (Hypocapnia: physiological effects).
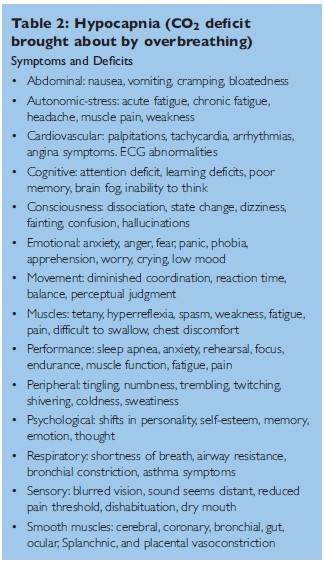
The symptoms and deficits caused by these physio logical changes can be profound, even devastating, and may include physical (eg brain fog), emotional (eg anger), cognitive (eg attention deficit), personality (eg sense of self), and behavioral (eg test taking) changes. Some of these symptoms and deficits (Fried, 1987, 1993; Laffey & Kavanagh, 2002) are listed in Table 2 (Hypocapnia: symptoms & deficits). These effects are all too often mistakenly attributed to other causes or are identified as “unexplained symptoms” by practitioners unaware of the impact of compromising breathing habits on health and performance.
These same physiological changes may also trigger (eg epilepsy), exacerbate (eg asthma), and prolong (eg nausea during pregnancy) symptoms and deficits of all kinds brought on independently by physical and psychological conditions unrelated to breathing. These interactive effects are almost invariably overlooked by practitioners and their clients. Examples of these conditions are listed in Table 3 (Hypocapnia: exacerbation of health issues and complaints).

Optimal respiratory health means maintaining a stable chemical axis of breathing wherein internal respiratory requirements are immediately and expeditiously addressed, despite the highly variable acrobatics of breathing mechanics during daily life that may be serving us in many other important ways such as talking. Aligning mechanics with chemistry, or not, addresses the most fundamental, practical, and profound factors that account for:
- the far-reaching debilitating effects of breathing habits that compromise respiratory chemistry, such as disturbed extracellular pH (eg blood plasma), deregulated electrolyte balance (eg bicarbonate), compromised blood flow (eg brain and heart), unfriendly hemoglobin (compromised delivery of O2), compromised muscle function (eg jaw tension and pain), fatigue, mood changes, and performance deficits (Fried, 1987, 1993; Laffey & Kavanagh, 2002, Maramattom & Wijdicks, 2015)
- the surprising benefits of breathing habits and breathing self-interventions that support optimal respiratory chemistry, such as improved physical performance (eg sports), symptom abatement (eg panic), improved cognition (learning, memory, and attention), enhanced task performance (eg test taking), successful management of emotions and stress (eg anxiety, anger), expanded consciousness (eg being present), improved self-awareness (eg sense of self), and better overall health (balanced pH chemistry).
Self-interventions and self-regulation
Self-interventions (techniques) are useful for managing, blocking, and avoiding dysfunctional breathing habits along with their troubling symptoms and deficits. Practitioners from diverse disciplines and perspectives focus on self-interventions for achieving beneficial outcomes that involve ‘doing the breathing’ in prescribed ways. One of the outcomes of prescriptive breathing, however, is not infrequently deregulated respiration, and unfortunately even the acquisition of dysfunctional habits where both practitioners and clients may misinterpret the outcomes and their associated physical and mental changes. This is because habits, ie the psychophysiology of breathing, are typically not identified and specifically addressed, nor is the alignment of so-called ‘good’ mechanics with healthy respiratory chemistry understood and evaluated.
Self-regulation is about identifying, disengaging, modifying, and/or replacing existing breathing habits with new ones. Useful solution-oriented interventions for learning new breathing habits are based on phenomenological exploration, the development of self-observation skills, and the principles of behavioral analysis including desensitisation, negative practice, cognitive learning, operant conditioning, CapnoLearnin, and multimodal biofeedback, eg CO2, HRV, and EMG. Simplistic mechanical solutions do not address psychological variables such as motivation and reinforcement, eg mouth breathing causes overbreathing. Mouth breathing, in fact, often restores good respiratory chemistry because it reduces air hunger and clears worry about getting enough oxygen.
Healthy breathing habits provide for self-regulation of mechanics in the service of respiratory chemistry, where self-intervention is not required, except when it is intentionally manipulated for reasons such as:
- identifying breathing habits and exploring their effects (ie breathing behavior analysis)
- exploring consciousness for personal awareness and therapeutic outcomes, eg holotropic breathing (Grof & Grof, 2010).
Self-regulatory breathing means ‘allowing the breathing’, unencumbered by unconscious habits and intentional manipulation, while simultaneously breathing for meeting other objectives, eg talking, meditating, relaxing, exploring. ‘Allowing’, although excellent advice often leading to temporary alignment of mechanics with chemistry, may also lead to ‘allowing’ unconsciously learned breathing habits (physiological reconfigurations) that need to be addressed first.
Respiration and consciousness
Hypocapnia (CO2 deficit) can result in radical cerebral vasoconstriction (Laffey & Kavanagh, 2002) leading to reductions in blood flow and volume of up to 40% to 50% or more within less than a minute (Brian, 1998). Oxygen and nitric oxide distribution by hemoglobin may be significantly compromised as per the Bohr Effect. Sodium and potassium ions migrate from cerebrospinal and interstitial fluids into neurons in exchange for hydrogen ions (H+), thus increasing neuronal metabolism, excitability, and contractility. All these factors together set the stage for brain hypoxia (oxygen deficit), brain hypoglycemia (glucose deficit), and metabolic (lactic) acidosis in neurons which may profoundly alter overall brain function in diverse ways, both subtle and obvious (Pardo & Miller, 2018; Laffey & Kavanagh, 2002).
The unfortunate outcomes of these physiological compromises include physical outcomes such as headache, ischemia, and the possible triggering of neurological syndromes as well as immediate effects on attention, perception, motivation, emotion, cognition, learning, memory, personality, performance, sense of self, and consciousness. It is these kinds of abrupt and disconcerting outcomes (Table 2) that motivate people to call 911 (emergency) for help (Fried, 1999).
Examples of psychological changes, from a downside perspective, include: emotional (deregulation) vulnerability, anxiety, anger, fear, panic, phobia, apprehension, worry, crying, low mood, dissociation, disorientation, dizziness, fainting, confusion, hallucinations, attention deficit, learning deficits, poor memory, brain fog, inability to think, low self-esteem, and undesirable shifts in personality (Fried, 1987; Fried & Grimaldi, 1993). On the other hand, from a consciousness perspective these kinds of ‘negatives’ can lay the groundwork for important ‘positives’ through individualized guided breathing explorations such as holotropic breathing.
The ways in which a specific person responds to these physiological changes are highly variable and are dependent on personal health, life circumstances, personality, immediate social environment, and especially personal psychological history. For example, disorientation and dizziness, as a function of oxygen deficit, may trigger fear or anxiety in one person and relief or relaxation in another. These differences are based on personal histories, including emotional, perceptual, and cognitive learning.
State change and dissociation are key to understanding how people respond to breathing mediated physiological changes. Breathing-induced states change may serve the individual in both positive and self-defeating ways, much in the same way as do psychoactive substances that provide for access and experience of self, others, and the world from new, different, and sometimes revealing perspectives. Intentional state change through over-breathing can set the stage for life-altering experiences, including:
- uncovering traumatic memories that provide for processing and reframing painful episodes in life
and/or
- discovering dysfunctional breathing habits and their associated effects triggered by specific places, times, people, tasks, emotions, thoughts, social circumstances, challenges, and physical feelings based on unique personal learning histories.
Unintentional breathing-mediated state changes, brought on by hypocapnia, are common. These state changes can serve people in powerful and unique ways, outside of their awareness, based on a personal history that gives specific meaning to such changes. These state changes can be habit-forming in the sense that they may provide for:
- avoidance of thoughts, emotions, and memories
or
- access to a different and preferable sense of self (personality). State-dependent learning and memory, and their role in drug addiction for example, have been extensively researched in both humans and animals and are described in thousands of articles in numerous behavioral science journals, eg Behavioural Pharmacology.
Concluding comments
Anyone who provides breathing education and/or training with clients can benefit immensely by knowing some of the basics of respiratory physiology and how changing breathing mechanics immediately, profoundly, and precisely alters respiratory chemistry. A truly practical understanding, however, of the dynamics of breathing physiology, how it is ultimately governed, how it affects us, and how we interact with it requires knowledge of its psychology, not just the details of its mechanics and chemistry.
Everyone has learned breathing habits, positive and negative. Habits are solutions triggered by specific experiences (stimuli) that are sustained by their outcomes (reinforcements). That is, breathing not only serves respiratory requirements (external respiration), but very importantly serves a host of other behavioral and psychological objectives, most of them unconscious. Examples of conscious objectives include: talking, emotional control, relaxation, meditation, psychotherapy, consciousness exploration, and cultivating self-awareness. Examples of unconscious objectives include: accessing secondary gain (eg headache), feeling in control, accessing emotions (eg anger) for controlling others, anxiety reduction, avoiding memories, disconnecting from challenges, and many others. Unconscious objectives are achieved through learning breathing habits based on specific experiences, eg feeling air hunger while wearing a mask during times of Covid. Everyone has learned breathing habits, self-enhancing or self-defeating, regulated by specific triggers based on their own personal histories.
Breathing mechanics and respiratory chemistry weave together in a dance. While embracing the daily diverse circumstances of our lives, breathing is designed to take care of us by aligning mechanics with chemistry in the service of health, performance, and consciousness. The ‘chemical axis’ of breathing generally remains within the optimal respiratory envelope, thus meeting oxygen, carbon dioxide, and acid-base balance requirements. Breathing habits that disturb the H-H equation, however, deregulate this dance. Assisting people with identifying and learning new breathing habits requires a detailed breathing behavior analysis where both the physiology and psychology of breathing are phenomenologically explored by clients with guidance from their practitioners.
The relationship between breathing and respiration, mechanics and chemistry, cannot be fully appreciated without understanding the psychological nature of physiology itself. Breathing, like any other behavior, is motivated and changes as a function of its outcomes. Breathing isn’t simply mindless automation of physiology to be somehow consciously manipulated in the name of self-help. It is truly so much more than this. Simply manipulating breathing physiology for well-intended purposes, without regard to its psychological nature, does not do justice to the richness and complexity of breathing.
References
Brian JE (1998) Carbon dioxide and the cerebral circulation. Anesthesiology, 88, 1365–1386.
Fried R (1999) Breathe well, be well. John Wiley & Sons.
Fried R (1987) Hyperventilation syndrome: research and clinical treatment. John Hopkins University Press.
Fried R & Grimaldi J (1993) The psychology and physiology of breathing in behavioral medicine, clinical psychology, and psychiatry. Plenum Press.
Grof S & Grof C (2010) Holotropic breathwork: a new approach to self-exploration and therapy. State University of York Press.
Gross SS & Lane P (1999) Physiological reactions of nitric oxide and hemoglobin: A radical rethink. Proceedings National Academy Science USA, 96 (18) 9967–9969.
Khoo MC (2011) Carbon dioxide and the control of breathing: a quantitative approach. In: Gravenstein JS, Jaffe MB, Gravenstein N & Paulus DA (eds) Capnograph. Cambridge University Press.
Laffey JG & Kavanagh BP (2002) Hypocapnia. New England Journal of Medicine, 34 (1) 43–53.
Levitzky MG (2007) Pulmonary physiology (7th edition). McGraw Hill.
Litchfield PM (2010) CapnoLearning: respiratory fitness and acid-base regulation. Psychophysiology Today, 7(1).
Litchfield PM (2017) Breathing: alignment of mechanics with chemistry. International Breath Foundation Newsletter, June.
Litchfield PM & Tsuda A (2006) Good breathing, bad breathing. L’Esprit D’aujourdhui, 8(1) 47–57.
Maramattom E & Wijdicks FM (2015) Neurology of pulmonology and acid-base disturbance. In: Schapira A, Byrne E, Frackowiak R, Mizuno Y & Silberstein S (eds) Neurology and Clinical Neuroscience. Mosby.
Pardo MC & Miller RD (2018) Basics of anesthesia (7th edition). Elsevier.
Thomson WST, Adams JF & Cowan RA (1997) Clinical acid-base balance. Oxford University Press.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}