
Tackling overdiagnosis: supporting the re-emergence of generalist expertise
Joanne Reeve, Associate Clinical Professor in General Practice,Warwick Medical School
Published in JHH12.3 – Beyond Peak Medicine
I am a generalist, GP and academic. My work tackles two of the biggest challenges facing modern healthcare systems. Namely, finding primary care solutions for the growing burden of chronic, complex illness, and building capacity for high-quality, meaningful primary care scholarship to support the necessary changes. I lead an international collaboration (SAGE) to develop, implement and evaluate the provision of the individually tailored model of care that is expert generalist practice. Our approach is underpinned by the principles of complex interventions, research and translational scholarship.As Chair of the Society for Academic Primary Care, I lead work to enhance the capacity for advancing primary care through education and research.All of which is sustained by my role as a non-principal GP in a busy inner city Liverpool practice.
Introduction
Overdiagnosis – the problem of too much medicine – is big business. Literally so, as described in the writing offered by the pharmaceuticalisation and medicalisation critiques (Williams et al 2011). Transforming ever more of human existence into a medical condition to be diagnosed and treated offers promise of ever greater market share to big companies around the world, but also figuratively speaking, if we look at the growing array of papers, journals, and conferences which discuss and debate the phenomenon. At the 2014 Preventing Overdiagnosis conference (www.preventingoverdiagnosis.net/ OD too much medicine), we held a Dangerous Ideas workshop (http://cmajblogs.com/dangerousideas/). The goal was to ignite some thinking about how we can tackle the problem of overdiagnosis by supporting the re-emergence of the expertise of the medical generalist. Some might consider this goal a dangerous idea in itself. In a world that places great value on specialist healthcare, and understands the generalist as ‘simply’ a ‘jack of all trades’, the idea may seem at best unintelligible and at worst ill-informed. In the workshop, we started by critically examining what it is to be a generalist. There are pages and pages written on this topic – although all too often they conflate the work that generalists do in our healthcare system (which is broad and diverse) with what it is to be an expert generalist (which is a distinct expertise). In particular, we focused on recognising that a generalist is an expert in assessing health needs. A generalist is an expert diagnostician. But we also considered that generalists do diagnosis differently. Their approach to making decisions about what is wrong (and so what needs doing) uses a different form of clinical reasoning to the diagnostic working of a specialist. It is this difference – but also the fact that it is poorly understood and so not trusted by non-generalists – that arguably contributed to the demise of the generalist; in particular, to the replacement of generalist diagnostic expertise with a technical bypass (Reeve et al 2013a), of which, more shortly. But it is this difference which has the potential to contribute to a reversal of the growing problems of overdiagnosis and treatment burden. Which musings sparked the beginning of some new thinking – about how we might support the continued re-emergence of expert generalist practice. Here, I will briefly describe the diagnostic expertise of the expert generalist and why I see it as at least part of the solution to overdiagnosis. I’ll describe some of my work looking at what is stopping people delivering generalist care at the front line, before telling you a bit about the dangerous ideas that came out of our workshop and how they link with some future directions of travel.
Rethinking the diagnostic process
If we want to tackle the problem of too much medicine, we need to think about how we define whether and when a person needs medical care. One way to define healthcare need is in terms of a person’s capacity to benefit from healthcare. We don’t need care if we wouldn’t benefit from its effects – there is no point in healthcare for healthcare’s sake. One example might be weighing patients in clinic – they have no need for care (weighing) if it does not benefit them. In today’s health system, healthcare need is most commonly defined by disease status (or increasingly by a ‘risk of disease’ status). The assumption is that if we have, or are at risk of, disease, then we need care. This shapes a diagnostic approach which asks, does this person have a disease (are they eligible for care), and is it medically safe to treat them (is care appropriate)? More than ten years ago, Tinetti and Fried (2004) proposed that we need to rethink our diagnostic (needs assessment) framework. They were among the first to highlight the now well recognised risks of overdiagnosis, treatment burden and underdiagnosis associated with an over focus on disease status in defining need (although we should of course recognise that the World Health Organization Alma Ata declaration effectively flagged this up in 1978, as have multiple authors since). Tinetti and Fried argued that we were reaching the ‘end of the disease era’. This was not a predication of eradication of disease, rather a recognition that this model of needs assessment was rapidly becoming less useful in an era characterised by chronic illness, multi-morbidty, and complexity. They called on healthcare to ‘abandon disease as the focus of medical care’ and instead seek the ‘identification and treatment of all modifiable biological and nonbiological factors’ Tinetti and Fried (2004). This approach recognises an alternative view of health – not as the absence of disease, but as a resource that people need and use for daily living. The goal for healthcare should therefore be ideally to support, but certainly not to undermine, health as a resource for daily living (HARFL) (Williamson and Carr 2009). This creates a different view of the process of medical needs assessment – defining medical need not by disease status, but by the potential impact of care on HARFL. Diagnosis is then about interpreting whether medical care, medicalising this individual’s health or illness experience, might or might not support HARFL. Iona Heath recognises this role in her Harveian lecture (2011), in which she describes the primary role of a generalist as a gatekeeper between illness and disease (see Figure 1).
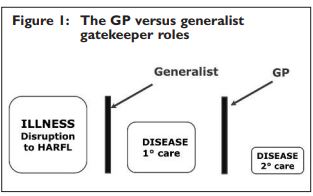
People experience illness (a disruption to health as a resource for daily living, HARFL), some of whom present to health services. Of these, a smaller proportion will be identified as having disease needing medical management in primary care (1º).A smaller portion again will have disease that needs specialist input (2º). We thus see two gatekeeper roles.The traditional gatekeeping role of the GP is in managing the interface between primary and secondary care. Heath recognised the distinct expertise of the medical generalist is as a gatekeeper between illness and disease – in deciding when it is in the best interests of this individual to intervene medically (Reeve et al 2012).
Viewed in this way, the decision to medicalise an illness experience becomes much more than deciding eligibility and appropriateness (as described previously). The generalist physician needs to know and understand the pros and cons for this individual of being on either side of the ‘medicalisation gate’. The expert generalist therefore needs to know about disease epidemiology in their population, medical diagnostic criteria, risks and prognosis associated with a diagnostic status, and the nature and impact of treatment options. But they also need to understand the pros and cons of remaining on the illness side of the gate; issues about resilience and salutogenesis, the non-medical resources available to an individual and a community to deal with illness experiences, as well as the immediate and longer term impact of iatrogenesis. The latter is more than the potential harms from side-effects of treatment, but also the impact of medicalisation on our understanding of health, wellbeing, the self, and our place in the world. For me, a key issue here is the extent to which medicalisation potentially undermines personal resilience – replaces an individual’s understanding of their role in managing illness with an expectation of a ‘technical fix’ from medical care (Reeve et al 2012). This is no easy task. And it is certainly not easy to describe, to standardise, to measure and so to fit in to the current workings of today’s health system. It is not readily understood by non-generalists. The failure to recognise this distinct expertise of the expert generalist – due in part by the failure of the profession to describe it – has contributed to the introduction of a ‘technical bypass’ (Reeve et al 2013a) of this form of decision-making in the form of decision aids, protocols, and governance targets to support adherence.
Describing generalist expertise
So our first task in supporting the re-emergence of generalist expertise is simply to describe what it is, and in a way that others can recognise. The Royal College of General Practitioners described generalism as expertise in whole person medical care (RCGP 2012). I expanded this in my description of generalism as an approach to care which is person not disease oriented; taking a continuous rather than an episodic view; integrating biomedical and biographical understanding of illness; to support decisions which recognise health as a resource for living and not an end in itself (Reeve et al 2013b). But we need to go further in describing what that means for the patient – in terms of how the expert generalist will understand, assess and intervene with their healthcare needs. And so we need to recognise that generalist practice is a form of interpretive practice – a way of providing explanation or meaning to a phenomenon, and so assessing and addressing healthcare need. I have therefore defined expert generalist practice as the critical, professional use of an appropriate range of knowledge (from both sides of the ‘gate’) in the dynamic exploration and interpretation of individual illness, in order to support and maintain health as a resource for living (Reeve 2010). Expert generalist practice therefore uses a different form of clinical reasoning to the medical diagnostic approach used by a medical specialist. Specialist reasoning adopts a deductive approach: applying a theory (of disease) to examine a phenomenon (of illness) and using a statistically informed approach to confirm or refute a hypothesis that this individual has this disease. Specialist deductive reasoning states how likely it is that a person has a disease. We assess the quality of deductive reasoning, and so specialist care, in terms of the precision and accuracy of our diagnostic reasoning – how often we get it ‘right’. By contrast, generalists use inductive reasoning. Starting with the phenomenon – an individual illness experience – exploring multiple elements in order to seek strong evidence (but not certain proof) of a broader theory. Generalists therefore seek to generate a defendable decision. Since generalist reasoning is built on an interpretive process (Reeve 2010), it can be described, and defended, with reference to the experience and expertise of other inductive, interpretive thinkers. Indeed, my work draws on the work of Maxwell to describe five key elements needed to generate a trustworthy interpretation (including a clear viewpoint from which we start, the data we use, the analysis we make, our quality check, and our evaluation of the utility of the decision) (Reeve 2010). Based on discussions with expert generalists, including those both teaching and learning the practice, I have therefore described a consultation model to help others recognise and practice as an expert generalist (Reeve 2015). The expert generalist diagnostic approach generates an individually tailored interpretation of the value and potential harm of medicalising an illness experience for this person and at this time. Generalist diagnosis therefore has potential to address the described problems of overdiagnosis, underdiagnosis and treatment burden.
Addressing barriers to expert generalist practice
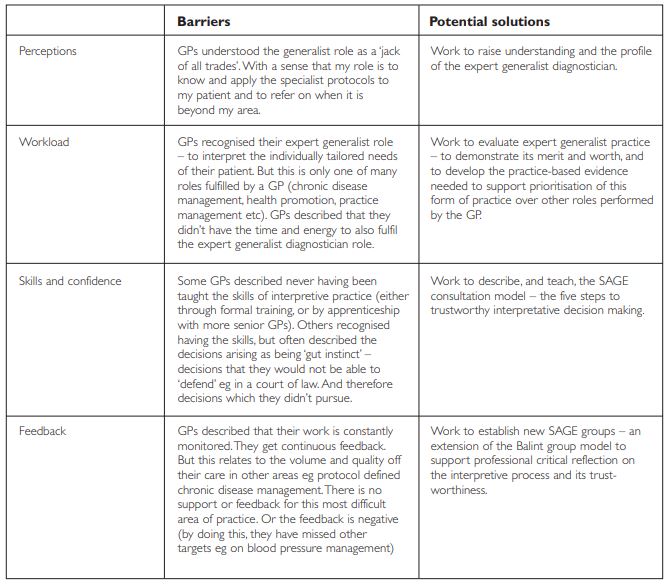
But the literature on overdiagnosis and treatment burden highlights that patients aren’t receiving expert generalist care, yet most of them will be seeing a GP. So why are GPs not delivering generalist care? This was a question we asked a couple of years ago (Reeve et al 2013b). Our study involved more than 200 GPs from around the UK, and from across multiple career stages. In a survey, focus groups and interviews, we asked GPs about the supports and barriers for working as an expert generalist – for applying their diagnostic expertise in whole person medical care. Four themes emerged describing barriers to expert generalist practice. In response, we are developing four areas of work. First raising the profile and understanding of the distinct expertise of the generalist; second finding creative ways to make space for expert generalist practice (Reeve and Bancroft 2014) including developing the research evidence that shows why it matters and should be prioritised; third teaching the expertise (the SAGE consultation model (Reeve 2015); and fourth providing feedback through SAGE groups (see Table 1).
Time for some dangerous ideas?
Returning to our Dangerous Ideas workshop… Having suggested that revitalising expert generalist practice might offer a way to address overdiagnosis, I invited the group to brainstorm their response to the question: “if you had 2 minutes in the lift with your health minister, what would you tell him/her to do differently in order to improve individually tailored healthcare?” The creative sparks flew! Each group pitched their idea back to the main group. Ideas included shifting the resources used to develop protocols to invest in expert generalist training; publishing research on individually tailored (generalist) care in the Daily Mail to mobilise the public voice; switch risk stratification approaches from assessing need for ‘extra’ care according to health service priorities (unplanned care use, disease status) to patient priorities (eg treatment burden related disruption to daily living). A show of hands vote (not consistent with any election regulatory standards!) identified ‘stop dictating (ie measuring) process of care so that the patient can choose their own path’ as the winner in the room on the day. The talk in the room was very much focused on the contextual and organisational factors limiting delivery of generalist care. But I might add in some dangerous ideas of my own. First, I would suggest that to embrace the opportunities to revitalise generalist practice, general practitioners need to change. We need ourselves to let go of the ‘jack of all trades’ model as the defining view of the generalist. Our approach to medical decision making means that we can be flexible in the problems we deal with – the range of patients and problems we see. But we are not defined by our diversity. Seeing a large range of patients, but only to deliver care technically defined by other people, does not make the best use of our expertise. We need as a profession to rethink what roles we should be doing, and what can and should be done by others (Reeve et al 2013c). At the same time as we rethink what the organisation of general practice will look like in the future, we also need to rethink what the professional practice of GPs will look like too. Second, we cannot assume that expert generalist practice will be the answer to the problems (just as we shouldn’t have assumed that specialist practice would). However I think we need new research models to help us critically but creatively develop and evaluate these new models of care. In Warwick, we are developing an approach to the coproduction of complex interventions. In this, we propose combining academic expertise in the development and interpretation of trustworthy knowledge with clinical expertise in the process of care clinical practice to co-create practice based evidence. We seek a trustworthy account of a practice-based view of a ‘way forward’ – describing options rather than definitive solutions.
GPs are the largest group of potentially practising generalists in the UK medical workforce. There is much concern about morale, recruitment and retention within the profession. Over the last two years, I have spent time with GPs, trainers and trainees talking about, and teaching the essentials of, expert generalist practice. I have left each event inspired by my colleagues – by their commitment to delivering high quality, individually tailored, whole person medical care; and by their enthusiasm for the opportunities the ideas described here offer them to revitalise the ways of working that brought them into general practice. The revitalisation of the generalist role heralds a new era for General Practice. Problems of too much medicine have brought us to this crisis point of a dangerously overstretched profession. But paradoxically, they may also prove to be the sparks that ignite a revitalisation of generalism and so of General Practice. You can find out more about generalism and our work to revitalise practice at our website: http://primarycarehub.org.uk/sage
References
- Heath I (2011) Divided we fail. Available at: https://www.rcplondon.ac.uk/sites/default/files/harveian-oration2011-web-navigable.pdf (accessed on 21 November 2015).
- Reeve J (2015) Supporting expert generalist practice: the SAGE consultation model. British Journal of General Practice 35 pp 207–208.
- Reeve J, Blakeman T, Freeman GK, Green LA, James P, Lucassen P, Martin CM, Sturmberg JP, van Weel C (2013a) Generalist solutions to complex problems: generating practice-based evidence – the example of managing multi-morbidity. BMC Family Practice 14 (112). DOI: 10.1186/1471-2296-14-112.
- Reeve J, Dowrick C, Freeman G, Gunn J, Mair F, May C, Mercer S, Palmer V, Howe A, Irving G, Shiner A, Watson J (2013b) Examining the practice of generalist expertise: a qualitative study identifying constraints and solutions. Journal of the Royal Society of Medicine, Short Reports 4: 2042533313510155.
- Reeve J, Irving G, Freeman G (2013b) Dismantling Lord Moran’s ladder: the primary care expert generalist. British Journal of General Practice 63 pp 34–35.
- Reeve J, Lynch T, Lloyd-Williams M, Payne S (2012) From personal challenge to technical fix: the risks of depersonalised care. Health and Social Care in the Community 20(2) pp 145–154.
- Reeve J (2010) Interpretive medicine: supporting generalism in a changing primary care world. London: Royal College of General Practitioners Occasional Paper Series, 88.
- Royal College of General Practitioners (2012) Medical generalism. Why expertise in whole person medicine matters. Available at: www.rcgp.org.uk/policy/rcgp-policy-areas/~/media/Files/Policy/A-Zpolicy/Medical-Generalism-Why_expertise_in_whole_person_ medicine_matters.ashx (accessed on 21 November 2015).
- Tinetti ME, Fried T (2004) The end of the disease era. The American Journal of Medicine 116(3) pp 179–185
- Williams SJ, Martin P, Gabe J (2011) The pharmaceuticalisation of society? A framework for analysis. Sociology of Health and Illness 33(5) pp 710–725.
- Williamson DL, Carr J (2009) Health as a resource for everyday life: advancing the conceptualisation. Critical Public Health 19(1) pp 107–122.


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}